Arch Iran Med. 28(12):710-718.
doi: 10.34172/aim.35112
Review Article
Exploring the Role of Central Venous Pressure in Cardiac Surgery-Associated Acute Kidney Injury: A Comprehensive Scoping Review
Maryam Aligholizadeh Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – original draft, 1 
Siavash Sangi Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Validation, Writing – review & editing, 1, *
Mehrdad Mesbah Kiaei Validation, Writing – review & editing, 2
Mahmoud Reza Mohaghegh Validation, Writing – review & editing, 3
Mohsen Abbasi Methodology, Writing – review & editing, 4
Melika Aligholizadeh Investigation, Visualization, 5
Author information:
1Department of Anesthesiology and Operating Room, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Anesthesiology and Pain Medicine, School of Medicine, Hasheminejad Kidney Center, Iran University of Medical Science, Tehran, Iran
3Department of Anesthesia, School of Medicine, and Hospital Management Research Center, Health Management Research Institute, Iran University of Medical Sciences, Tehran, Iran
4Department of Anesthesia and Critical Care, Hasheminejad Hospital, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
5Department of Laboratory Sciences, Langroud School of Allied Medical Sciences, Guilan University of Medical Sciences, Langroud, Iran
Abstract
Background:
Acute kidney injury (AKI) is a critical complication, affecting up to 30% of coronary artery bypass grafting (CABG) patients, and contributing to significant morbidity and mortality. Recent studies indicate that increased central venous pressure (CVP) might significantly contribute to the development of AKI by causing venous congestion and impairing renal blood flow. However, the association between CVP and AKI in patients undergoing CABG has not been thoroughly investigated. This scoping review evaluates the current evidence on CVP as a hemodynamic marker associated with AKI in adults undergoing cardiac surgery with cardiopulmonary bypass (CPB), with a particular focus on CABG where reported.
Methods:
This scoping review, conducted over 12 weeks, followed the PRISMA-ScR guidelines and Arksey and O’Malley framework. A systematic search of PubMed, Scopus, Web of Science, and MEDLINE (2016–2024) identified studies on adult CPB-supported cardiac surgery, including CABG. Eligible studies reported quantitative CVP (intra- or postoperative) and standardized AKI criteria. No formal bias assessment was performed; data extraction was independently conducted by two reviewers using a standardized form.
Results:
Of 1,717 studies screened, 16 met the inclusion criteria, mostly retrospective cohorts involving CABG patients. Overall, elevated CVP showed a positive association with postoperative AKI, though thresholds varied (intraoperative 6.5–12 mm Hg; postoperative>6.6–10.3 mm Hg). Several studies revealed a synergistic effect between high CVP and low mean arterial pressure (MAP). Despite consistent trends, heterogeneity in design and CVP assessment limits comparability. Most studies used the KDIGO criteria for AKI definition.
Conclusion:
High CVP is commonly linked to the occurrence of AKI in patients undergoing cardiac surgery. The evidence mapped in this review suggests a potential role for CVP monitoring in perioperative care, though clinical recommendations require validation through prospective trials. Future research should focus on establishing standardized CVP thresholds and evaluating their utility in AKI risk stratification.
Keywords: Acute kidney injury, Central venous pressure, Coronary artery bypass grafting
Copyright and License Information
© 2025 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Aligholizadeh M, Sangi S, Mesbah Kiaei M, Mohaghegh MR, Abbasi M, Aligholizadeh M. Exploring the role of central venous pressure in cardiac surgery-associated acute kidney injury: a comprehensive scoping review. Arch Iran Med. 2025;28(12):710-718. doi: 10.34172/aim.35112
Introduction
With global advancements in living standards and rising life expectancy, the prevalence of coronary artery disease (CAD) has increased markedly. Coronary artery bypass grafting (CABG) remains a cornerstone intervention for patients with advanced CAD and other complex cardiovascular conditions, significantly improving survival and quality of life. However, like other major cardiac surgeries involving cardiopulmonary bypass (CPB), including valve replacement and aortic repair, CABG is associated with a substantial risk of postoperative complications.1,2 Acute kidney injury (AKI) is among the most common and serious complications following cardiac surgery. According to recent research, the incidence of cardiac surgery-associated AKI (CSA-AKI) varies between 10% and 40%, depending on the diagnostic criteria used. The development of CSA-AKI has been associated with a 3–8-fold increase in mortality, longer durations of intensive care and overall hospital stay, as well as elevated healthcare costs.3 Cardiac surgery poses unique challenges, including CPB, aortic cross-clamping, high-volume blood transfusions, and extensive use of vasopressors.4,5 These factors disrupt renal perfusion, trigger ischemia-reperfusion cycles, and promote oxidative stress and inflammation, all of which play a role in AKI development. Historically, renal hypoperfusion has been viewed as the dominant hemodynamic mechanism contributing to AKI, leading clinicians to focus primarily on maintaining adequate mean arterial pressure (MAP) and cardiac output. Although a MAP ≥ 65 mm Hg is commonly targeted to reduce AKI risk, recent evidence suggests that perfusion pressure alone may not fully explain postoperative renal dysfunction.6,7 Cardiac surgery entails unique insults—including CPB, aortic cross-clamping, massive transfusions, and vasopressor support—that collectively compromise renal perfusion, drive ischemia-reperfusion injury, and amplify oxidative stress and inflammation.8,9 Emerging evidence now highlights venous congestion as an equally important yet underrecognized factor in CSA-AKI pathophysiology. Elevated central venous pressure (CVP), an indicator of venous congestion, directly contributes to renal venous hypertension and reduces the renal arteriovenous pressure gradient.10,11 This hemodynamic alteration impairs renal blood flow, decreases glomerular filtration rate, and exacerbates intrarenal pressure. Elevated CVP activates both the sympathetic nervous system and the renin–angiotensin–aldosterone system, leading to increased sodium reabsorption, fluid accumulation, and heightened systemic inflammatory responses.6,12
Despite the widespread use of CVP monitoring during and after cardiac surgery, there remains no consensus on the threshold values at which CVP becomes deleterious to renal function in CABG patients.13,14 Moreover, the relative impact of intraoperative versus postoperative CVP elevations has not been systematically synthesized, and it is still unclear whether CVP acts as an independent predictor of CSA-AKI or merely reflects other hemodynamic derangements such as right ventricular dysfunction or volume overload.13,15 These uncertainties underscore the need for comprehensive evidence mapping in this domain. The rationale for this scoping review is to systematically chart and synthesize the available literature regarding CVP and its association with AKI following CABG and other cardiac surgeries, identifying existing knowledge gaps and research trends. By applying the Population–Concept–Context (PCC) framework, this review focuses on adult patients undergoing cardiac surgery (Population), explores the concept of CVP monitoring as a potential predictor or contributing factor to AKI (Concept), and examines its application and implications across intraoperative and postoperative settings (Context). This scoping review critically examines the available evidence on CVP’s association with AKI in this population, aiming to elucidate its clinical utility, limitations, and potential as a hemodynamic marker. By bridging this knowledge gap, the review offers insights that could refine perioperative management strategies and improve renal outcomes in cardiac surgery patients (Figure 1).

Figure 1.
Graphical Abstract: Central venous pressure and cardiac surgery-associated acute kidney injury – a scoping review
.
Graphical Abstract: Central venous pressure and cardiac surgery-associated acute kidney injury – a scoping review
Study Design
This scoping review was carried out over an intensive 12-week period. Although the timeline was accelerated, methodological rigor and accuracy were consistently upheld. The review process was structured according to Arksey and O’Malley’s scoping review framework16 and aligned with the PRISMA-ScR reporting criteria.9,17 We implemented the five core phases described by Arksey and O’Malley16,18:
-
Stage 1: Defining the study objectives and formulating the key research questions;
-
Stage 2: Conducting a comprehensive search to locate relevant literature;
-
Stage 3: Screening and selecting studies based on the established criteria;
-
Stage 4: Systematically charting and organizing the extracted data;
-
Stage 5: Integrating, synthesizing, and presenting the findings.
This scoping review was conducted between October and December 2024 and adhered to the methodological framework proposed by Arksey and O’Malley, with additional refinement using the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) checklist to enhance transparency and methodological rigor. A scoping review represents a systematic approach to mapping the extent, range, and nature of research evidence on a given topic, rather than establishing causal relationships or evaluating intervention effectiveness. This approach is particularly appropriate when the existing literature is heterogeneous or inconclusive, as is the case with CVP and its relationship to postoperative renal outcomes. Although CVP is routinely monitored in cardiac surgical practice to assess fluid status and cardiac function, its specific role in predicting AKI following CABG remains underexplored. Accordingly, this review sought to map and synthesize current evidence regarding the association between CVP and AKI in adult patients undergoing CABG — either isolated or combined with minor concurrent procedures. By identifying key patterns, methodological limitations, and knowledge gaps across existing studies, this scoping review aims to inform future research directions and support the development of evidence-based strategies to improve perioperative management and renal outcomes in CABG patients.19,20
The scope of this review was established using the Population–Concept–Context (PCC) framework:
-
Population: Adult patients undergoing cardiac surgery, including isolated CABG and CABG combined with valve procedures, while excluding isolated valve or aortic operations.
-
Concept: CVP thresholds and the timing of their assessment (before, during, and after surgery) in relation to the onset of AKI.
-
Context: Perioperative cardiac surgery settings encompassing intraoperative care and postoperative management in intensive care units.
-
Outcome: Incidence and severity of AKI based on standardized diagnostic criteria such as KDIGO, RIFLE, or AKIN.
-
Study Design: Observational studies (including prospective and retrospective cohorts) and randomized controlled trials (RCTs) were considered to provide comprehensive coverage of the existing evidence.
This design enabled mapping of evidence across study types, identifying the extent of current knowledge and highlighting the methodological limitations that influence interpretation of CVP–AKI associations.
Research Questions
For this scoping review, the following research questions were formulated:
-
What is the association between elevated CVP and development of AKI in adult patients undergoing cardiac surgery, with particular focus on CABG performed alone or in combination with valve procedures?
-
Which perioperative CVP thresholds (measured preoperatively, intraoperatively, or postoperatively) are most strongly associated with the incidence and severity of AKI following cardiac surgery?
-
How do the timing, duration, and magnitude of CVP elevation influence renal outcomes and recovery trajectories in this population?
-
What implications do these findings have for integrating CVP monitoring into perioperative hemodynamic management protocols to prevent or mitigate CSA-A?
Search Strategy
An independent preliminary search was conducted across major scholarly databases, including Scopus, Web of Science, PubMed, and MEDLINE. The MeSH headings and keywords used in the search strategy included: AKI (renal failure, renal insufficiency), cardiac surgery (heart surgery, cardiovascular surgical procedure, coronary bypass surgery, coronary artery surgery), and CVP. The incorporation of synonyms and related terms expanded the scope of the search. Boolean operators (AND, OR) and truncation symbols were used to combine and expand search terms appropriately. To maximize retrieval of relevant literature, the reference lists of all included studies were manually screened to identify additional eligible publications. Initial screening was based on titles and abstracts to exclude studies that did not meet the eligibility criteria. Any discrepancies in selection were resolved through discussion among the four reviewers, with final inclusion decisions made by consensus. Data were systematically extracted from all selected studies using a standardized form, capturing key elements such as authorship, study objectives, participant characteristics, interventions (where applicable), outcomes, and main findings. The search strategy focused on studies published between January 2016 and December 2024 to ensure relevance to contemporary clinical practice.
Study Selection
The screening process was performed by pairs of authors who independently reviewed the titles, abstracts, and full texts of the retrieved studies. Study selection was guided by predetermined inclusion and exclusion criteria. A pre-designed data collection form was utilized, which was pilot-tested by two reviewers using four articles. No discrepancies were identified during the data extraction process.
Inclusion and Exclusion Criteria
Studies were included if they fulfilled the predefined eligibility criteria outlined below:
-
Population: Adult patients (aged ≥ 18 years) undergoing isolated CABG or CABG combined with minor concomitant procedures, excluding those involving primary valve replacement/repair or major aortic surgery.
-
Outcome: Reporting of AKI incidence defined using standardized diagnostic criteria, primarily the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.
-
Study design: Observational studies (prospective or retrospective cohorts) or randomized controlled trials published between January 2016 and December 2024.
-
Language: Full-text articles published in English.
Exclusion Criteria Comprised
-
Studies without a clearly specified AKI definition,
-
Those lacking sufficient data on CVP measurements,
-
Research conducted in pediatric populations or non-cardiac surgical settings,
-
Narrative reviews, editorials, commentaries, and non-peer-reviewed publications.
-
All identified articles were imported into EndNote version 9 for reference management, and duplicate records were systematically removed.
Two screening phases followed: initially, three independent reviewers evaluated titles and abstracts against the eligibility criteria. In the second phase, full texts were assessed for final inclusion. Any disagreements were resolved through discussion, with a fourth senior researcher making the final adjudication when consensus could not be reached.
Data Extraction and Synthesis
All screening stages—title, abstract, and full-text—were conducted independently by two reviewers in duplicate, and data extraction was cross-verified by a second reviewer to ensure comprehensiveness and transparency. Any disagreements were resolved through discussion, and unresolved issues were adjudicated by a third senior reviewer. The workflow and reviewer assignments were managed using Covidence systematic review software, ensuring traceability and minimizing bias. Each included study was reviewed to capture the following data fields:
-
Bibliographic information: authors, publication year, country, and study design.
-
Study population: sample size, demographic characteristics, and type of cardiac surgery (isolated CABG or CABG with minor valve procedures).
-
Clinical parameters: CVP measurement protocols (timing, duration, and threshold values), perioperative monitoring phase (pre-, intra-, or postoperative), and fluid management strategies.
-
Outcome measures: definitions and diagnostic criteria for AKI, including KDIGO, RIFLE, or AKIN classifications, and reported clinical outcomes such as AKI incidence, severity, renal recovery, mortality, and ICU/hospital length of stay.
A structured Excel data extraction template was employed to maintain uniformity and minimize potential subjective bias. Extracted data were summarized in tabular format to facilitate cross-study comparison.
In line with the methodological principles of scoping reviews, we did not conduct a formal quality assessment or evaluate the risk of bias. Rather, we employed a narrative and thematic synthesis, guided by the Arksey and O’Malley framework and the PRISMA-ScR reporting standards. The studies were grouped thematically according to (1) the phase of CVP monitoring (pre-, intra-, or postoperative), (2) the reported relationship between CVP elevation and AKI, and (3) the methodological diversity across studies. This structured synthesis enabled the identification of key evidence patterns and knowledge gaps, forming a robust foundation for future research recommendations.
Results
This scoping review study was conducted during the second half of 2024. The initial search identified 1,717 studies. After removing 552 duplicates, a total of 1,165 studies remained. Following title screening, 1,017 studies were excluded. The abstracts of the remaining 338 studies were reviewed. From the abstract review, 241 studies focused exclusively on postoperative AKI following CABG without addressing the role of CVP; 97 studies investigated the impact of CVP on patient mortality but did not discuss AKI outcomes. Consequently, 148 studies were selected for full-text review. Of these, 23 studies had inaccessible full texts, 3 studies addressed pediatric anesthesia, which was beyond the scope of this review, 5 studies were published in languages that did not meet the inclusion criteria, 42 studies discussed preoperative AKI exclusively, and 59 studies explored factors contributing to postoperative AKI but did not provide relevant results. Ultimately, 16 studies met the final inclusion criteria (Figure 2). These studies defined postoperative AKI using specific and standardized criteria; reported on CVP measurement time points and evaluated the association between CVP and AKI outcomes; and specifically focused on patients undergoing CABG surgery (Table 1).
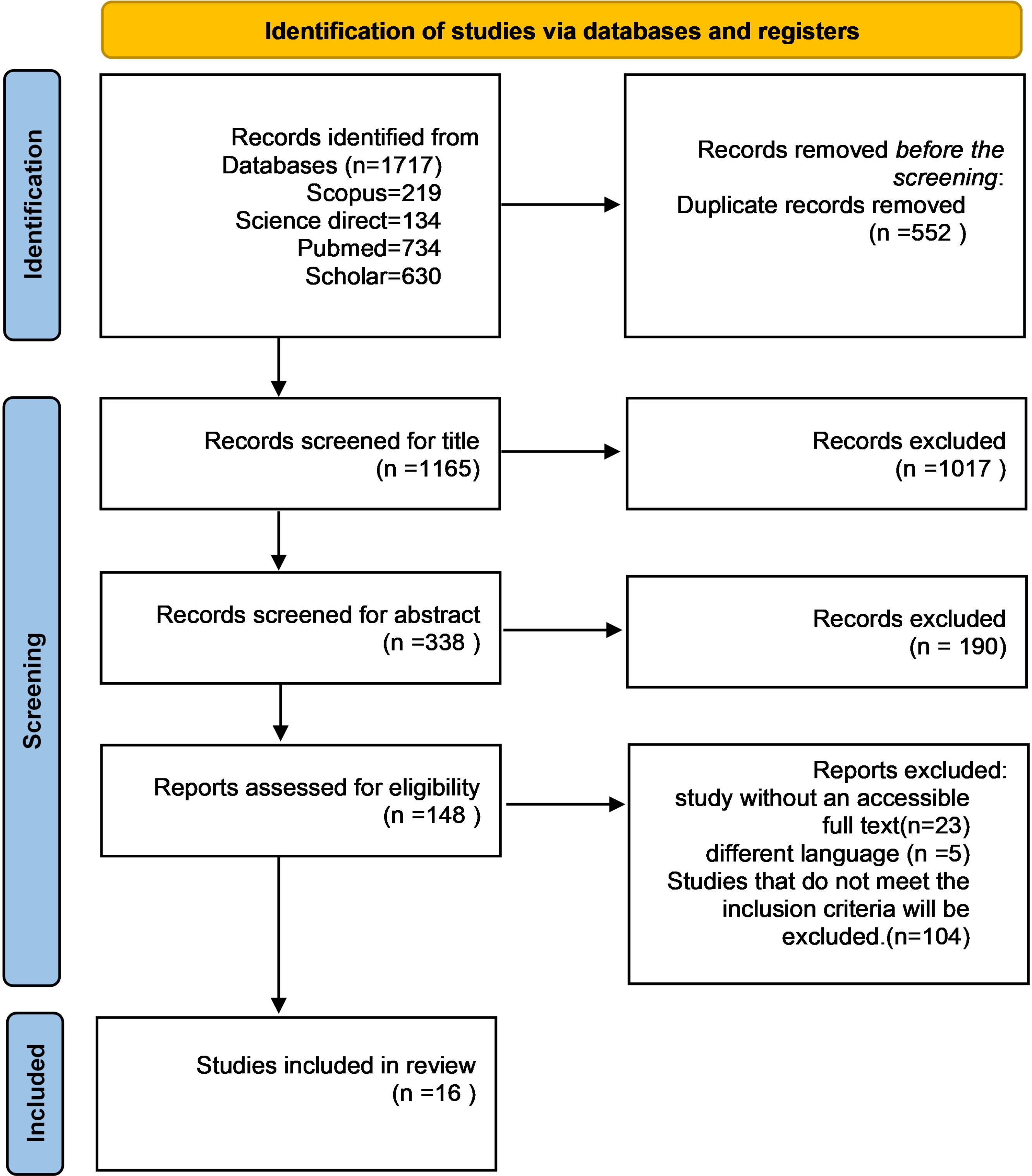
Figure 2.
Flow Chart the Literature Search Strategy
.
Flow Chart the Literature Search Strategy
Table 1.
Summary of Studies Discussing the Relationship Between Central Venous Pressure and the Incidence of Renal Failure After CABG
Year/
Author
|
Country/center
|
Study Design
|
Sample size (n), population
|
CVP measurement (timing & threshold)
|
AKI criteria
|
Main findings
|
| 2024, Demirjian et al21 |
USA |
A Retrospective Cohort Study |
60,424 cardiac surgery patients (CABG, valve, aorta( |
Post-closure & ICU admission; continuous pulmonary artery catheter measurements |
The primary outcome was the occurrence of moderate to severe AKI, defined as stage 2 or higher according to the modified KDIGOa creatinine-based criteria, within a 14-day period following surgery. |
Elevated CVP + low MAP → synergistic ↑AKI risk (P = 0.009) |
| 2024. Wang et al5 |
China |
A Retrospective Cohort Study |
2,048 cardiac surgeries with CPB |
Intra-CPB; high CVP ≥ 6.5 mm Hg |
KDIGO |
High CVP ( ≥ 6.5 mm Hg) independently predicted AKI (P = 0.017) |
| 2023, Dang et al22 |
USA |
A retrospective cohort study |
23 cardiac surgery adults |
Pre-CPB & ICU; dynamic |
KDIGO |
↑CVP → ↓effective renal perfusion pressure → ↑AKI (P < 0.05) |
| 2022, Alhulaibi et al23 |
Saudi Arabia |
A Retrospective Cohort Study |
329 cardiac surgery with CPB |
Post-op CVP via PAC |
KDIGO |
AKI group CVP = 11.5 ± 2.7 > controls (10.4 ± 2.5 mm Hg) (P = 0.003) |
| 2022, Tohi et al24 |
Japan |
A prospective observational study |
64 CPB surgeries |
Intra-op continuous PAC |
KDIGO |
Dynamic ↑CVP strongly correlated with AKI (P < 0.0001) |
| 2021, Neuman et al25 |
Australia |
An observational cohort study |
221 cardiac surgeries |
Post-op ICU |
KDIGO |
CVP ≥ 9 mm Hg→ ↑AKI risk (P = 0.01) |
| 2021, Lopez et al26 |
USA |
An observational cohort study |
425 elective CABG/valve/aorta |
Intra-op continuous CVP (excluding CPB) |
KDIGO |
↑CVP (60 mm Hg/min) → 6–30% higher AKI risk (P = 0.008) |
| 2021, Kotani et al27 |
Japan |
A multicenter retrospective cohort study |
746 CABG/valve |
Pre- & post-op CVP (1h intervals, 24 h) |
KDIGO |
↑time-weighted CVP → AKI progression OR 1.12 (P = 0.0013) |
| 2020, Chen et al14 |
China |
A Retrospective Cohort Study |
5,127 CABG/valve |
Pre/post-CPB CVP (12–20 mm Hg thresholds) |
KDIGO |
Venous congestion > hypotension in AKI prediction |
| 2020, Farghaly et al28 |
Egypt |
A Prospective Observational Study |
100Post-cardiac vasopressor patients post operative |
Pre- & post-op CVP (24 h mean) |
KDIGO |
↑CVP → 50% AKI incidence (P < 0.001) |
| 2019, Raymond Hu el29 |
Australia |
A retrospective, observational cohort study |
664 CPB |
Baseline & post-induction CVP |
AKI was defined by a > 50% rise in serum creatinine from baseline within 7 postoperative days, per RIFLEb criteria. |
Baseline CVP → independent AKI predictor, along with factors like age, preoperative creatinine, and LV dysfunction (P < 0.05). |
| 2019, Jin et al30 |
China |
A retrospective analysis |
300 post-cardiac surgery |
Post-op 24 h CVP |
KDIGO |
Patients with AKI exhibited significantly higher CVP values, both at peak (10.7 ± 3.5 vs. 9.8 ± 2.7 mm Hg) and nadir (5.0 ± 2.2 vs. 4.5 ± 1.8 mm Hg), compared to those without AKI (P < 0.05). |
| 2019, Che et al31
|
China |
Observational study |
2,552 mixed cardiac |
Post-op CVP < 4.4 or > 10.3 cmH₂O |
KDIGO |
CVP of less than 4.4 mm Hg or greater than 10.3 mm Hg in the postoperative period→ ↑AKI risk (P < 0.001). |
| 2018, Jiang et al32 |
China |
A propensity
score-matched case-control study |
1,773 CABG/valve |
Postoperative CVP was extracted from the cardiac surgery database of Zhongshan Hospital |
KDIGO |
CVP > 7.35 mm Hg at ICU admission independently predicted AKI-RRT after cardiac surgery (OR = 1.6 per 1 mm Hg increase; P < 0.05). |
| 2018, Beaubien-Souligny et al33 |
Canada |
A prospective observational cohort study |
145 CABG/CPB |
Post-op CVP continuous |
KDIGO |
↑CVP → ↑AKI risk (with a hazard ratio 1.04 per mm Hg) (P = 0.02). |
| 2017, Jiang et al34
|
China |
A retrospective cohort study |
1,587 CABG/valve |
Post-op ICU CVP |
KDIGO |
AKI group )8.0 ± 2.1 mm Hg vs. 6.2 ± 2.0 mm Hg (P < 0.01) |
aKidney Disease: Improving Global Outcomes (KIDGO) defined as: (1) ΔCr ≥ 0.3 mg/dL within 48 h, (2) Cr ≥ 1.5 × baseline within 7 days, or (3) urine output < 0.5 mL/kg/h for > 6 h 5.
bThe RIFLE classification, proposed by Bellomo et al, defines the first stage of AKI as a decrease of more than 25% in the estimated glomerular filtration rate (GFR).23,35
Across the studies, associations between elevated CVP and AKI were generally positive but varied in magnitude and threshold (ranging 6.5–12 mm Hg intraoperatively, > 6.6–10.3 mm Hg postoperatively). Variability in AKI definitions (KDIGO, RIFLE, AKIN) and timing of CVP assessment contributes to the heterogeneity. The included studies primarily involved adult patients undergoing CABG, either isolated or combined with minor concomitant procedures, with CVP measured intraoperatively or postoperatively.
To ensure transparency and reproducibility, only peer-reviewed articles meeting predefined inclusion criteria were considered. All study selection decisions were documented, and inter-rater agreement during screening and full-text review was high (Cohen’s kappa > 0.80), ensuring consistency across reviewers. No formal risk-of-bias or quality assessment was conducted, in line with scoping review methodology.
The results indicate that elevated CVP is frequently associated with postoperative AKI. Studies consistently demonstrated that higher CVP, particularly when combined with other hemodynamic factors such as low MAP, increased the likelihood of AKI. However, differences in CVP measurement protocols, threshold values, and AKI classification systems highlight the need for standardized definitions and measurement practices in future research. These findings underscore the potential role of CVP monitoring in perioperative care and provide a foundation for future prospective studies aimed at developing CVP-guided strategies to mitigate postoperative renal complications in CABG patients.
Summary of Evidence
This scoping review synthesizes evidence regarding the potential predictive role of CVP for AKI following CABG. The included studies provide valuable insight into the relationship between CVP and AKI incidence, examining both measurement timing and the magnitude of association. However, across the studies, the findings are heterogeneous with respect to CVP thresholds, measurement timing, and AKI definitions. CVP thresholds associated with increased AKI risk varied widely (6.5–14 mm Hg intraoperatively, 6.6–12 mm Hg postoperatively), and some studies reported weak or non-significant associations (Table 1).5,14,25,31 Most studies used KDIGO guidelines, though RIFLE and other non-standard definitions were also applied.29
Principal Findings
Elevated CVP consistently emerged as an independent predictor of postoperative AKI across diverse patient populations and study designs. CVP thresholds associated with increased AKI risk varied, ranging from 6.5 mm Hg to ≥ 12 mm Hg, with postoperative CVP measurements showing the strongest association. According to the studies referenced, elevated CVP was found to significantly contribute to an increased risk of AKI, which in turn was associated with higher mortality rates.5,14,25,30,31,34
Although all included studies demonstrated a significant relationship between elevated CVP and the occurrence of AKI, there was substantial variability in the CVP cutoff values used, the timing of measurements (intraoperative versus postoperative), and the magnitude of the reported associations. This heterogeneity suggests that CVP is not a universally applicable predictor and cautions against broad clinical recommendations in the absence of standardized protocols.
Venous congestion may contribute to renal dysfunction through several mechanisms:
-
Reduced renal perfusion pressure: Elevated CVP decreases the renal arteriovenous pressure gradient, impairing glomerular filtration and renal blood flow.26
-
Intrarenal congestion: Increased intrarenal pressure from elevated CVP directly contributes to structural and functional renal impairment.7,26
-
Neutrophil accumulation: High CVP can impede renal blood flow, leading to neutrophil accumulation in peritubular capillaries and upregulation of inflammatory signals, potentially causing kidney damage.5
Moreover, the review highlighted a synergistic relationship between elevated CVP and low MAP, wherein the combination significantly increased AKI risk. This finding emphasizes the need for balanced hemodynamic management, targeting both arterial and venous pressures, to mitigate renal complications.21
Clinical Implications
While CVP monitoring may provide useful information for perioperative risk assessment in CABG patients, the current evidence does not support a uniform CVP threshold or routine use to guide interventions in isolation. Interventions such as fluid management, inotropes, or diuretics should be individualized based on patient-specific risk factors, intraoperative events, and postoperative hemodynamic status.5,12,14,21,26,36
Study Strengths and Limitations
We excluded studies published prior to 2016 to reduce the risk of temporal bias. This review is strengthened by the use of a systematic approach, compliance with PRISMA-ScR reporting standards, and the incorporation of heterogeneous study populations, all of which improve the overall applicability of the results. However, the review is limited by its reliance on observational data, heterogeneity in CVP measurement techniques, timing, and thresholds, variability in AKI definitions, and differences in patient populations and surgical practices. Additionally, only studies published in English were included, introducing potential language bias.
Despite the consistency of findings, significant heterogeneity complicates direct comparison across studies. Some studies utilized intraoperative CVP monitoring37,38, while others focused on postoperative values,25,30 leading to variability in reported associations with AKI. These studies reported various CVP thresholds associated with an increased risk of AKI; however, they did not establish a precise or definitive CVP range. Furthermore, most studies rely on retrospective cohort designs, which limit causal inference.
Future Directions
Several avenues for future research emerge from this review:
-
Standardization of CVP measurement and reporting protocols to reduce heterogeneity.
-
Investigation of optimal CVP thresholds predictive of AKI in multicenter prospective studies.
-
Integration of CVP into broader risk models, including MAP, cardiac output, and fluid balance.
-
Intervention studies evaluating CVP-guided perioperative strategies, such as targeted fluid or diuretic
Conclusion
This scoping review maps and synthesizes current evidence on the association between CVP and AKI following cardiac surgery. Across the included studies, elevated CVP was generally associated with a higher risk of postoperative AKI, although thresholds, measurement timing, and AKI definitions varied.These findings highlight the potential role of CVP monitoring in perioperative hemodynamic management but do not establish causality due to observational study designs and methodological heterogeneity. Prospective, multicenter studies with standardized CVP protocols are needed to confirm these associations, identify optimal thresholds, and evaluate CVP-guided interventions to improve renal outcomes in CABG patients.
Competing Interests
The authors declare that they have no relevant conflicts of interest related to this publication.
Ethical Approval
Ethical approval was not required for this scoping review, as it synthesizes findings from existing, publicly available literature and does not involve primary data collection, human subjects, or animal experimentation.
Funding
This study received no external funding. The authors report no financial relationships relevant to this work.
References
- Zhang WY, Wu WL, Gu JJ, Sun Y, Ye XF, Qiu WJ. Risk factors for postoperative delirium in patients after coronary artery bypass grafting: a prospective cohort study. J Crit Care 2015; 30(3):606-12. doi: 10.1016/j.jcrc.2015.02.003 [Crossref] [ Google Scholar]
- Parthasarathi G, Raman SP, Sinha PK, Singha SK, Karunakaran J. Ketamine has no effect on oxygenation indices following elective coronary artery bypass grafting under cardiopulmonary bypass. Ann Card Anaesth 2011; 14(1):13-8. doi: 10.4103/0971-9784.74394 [Crossref] [ Google Scholar]
- Harky A, Joshi M, Gupta S, Teoh WY, Gatta F, Snosi M. Acute kidney injury associated with cardiac surgery: a comprehensive literature review. Braz J Cardiovasc Surg 2020; 35(2):211-24. doi: 10.21470/1678-9741-2019-0122 [Crossref] [ Google Scholar]
- Al-Githmi IS, Abdulqader AA, Alotaibi A, Aldughather BA, Alsulami OA, Wali SM. Acute kidney injury after open heart surgery. Cureus 2022; 14(6):e25899. doi: 10.7759/cureus.25899 [Crossref] [ Google Scholar]
- Wang L, Hu L, Yan Dai Q, Qi H, Wang Z, Chen X. Intraoperative central venous pressure during cardiopulmonary bypass is an alternative indicator for early prediction of acute kidney injury in adult cardiac surgery. J Cardiothorac Surg 2024; 19(1):262. doi: 10.1186/s13019-024-02734-7 [Crossref] [ Google Scholar]
- Husain-Syed F, Gröne HJ, Assmus B, Bauer P, Gall H, Seeger W. Congestive nephropathy: a neglected entity? Proposal for diagnostic criteria and future perspectives. ESC Heart Fail 2021; 8(1):183-203. doi: 10.1002/ehf2.13118 [Crossref] [ Google Scholar]
- Chen X, Wang X, Honore PM, Spapen HD, Liu D. Renal failure in critically ill patients, beware of applying (central venous) pressure on the kidney. Ann Intensive Care 2018; 8(1):91. doi: 10.1186/s13613-018-0439-x [Crossref] [ Google Scholar]
- Ferreira LO, Vasconcelos VW, Lima JS, Vieira Neto JR, da Costa GE, Esteves JC. Biochemical changes in cardiopulmonary bypass in cardiac surgery: new insights. J Pers Med 2023; 13(10):1506. doi: 10.3390/jpm13101506 [Crossref] [ Google Scholar]
- Hardiman SC, Villan Villan YF, Conway JM, Sheehan KJ, Sobolev B. Factors affecting mortality after coronary bypass surgery: a scoping review. J Cardiothorac Surg 2022; 17(1):45. doi: 10.1186/s13019-022-01784-z [Crossref] [ Google Scholar]
- Matsuto K, Maruichi-Kawakami S, Aida K, Imamoto K, Yukawa H, Kanazawa T. Prognostic implications of post-discharge hemodynamic congestion assessed by peripheral venous pressure among patients discharged from acute heart failure. Int J Cardiol 2023; 374:58-64. doi: 10.1016/j.ijcard.2022.12.057 [Crossref] [ Google Scholar]
- Zhang H, Lian H, Zhang Q, Zhao H, Wang X. Can central venous pressure help identify acute right ventricular dysfunction in mechanically ventilated critically ill patients?. Ann Intensive Care 2024; 14(1):114. doi: 10.1186/s13613-024-01352-9 [Crossref] [ Google Scholar]
- Li J, Wang R, Wan J, Zhu P, Xiao Z, Wang X. Postoperative central venous pressure is associated with acute kidney injury in patients undergoing coronary artery bypass grafting. Front Cardiovasc Med 2022; 9:1016436. doi: 10.3389/fcvm.2022.1016436 [Crossref] [ Google Scholar]
- Chen CY, Zhou Y, Wang P, Qi EY, Gu WJ. Elevated central venous pressure is associated with increased mortality and acute kidney injury in critically ill patients: a meta-analysis. Crit Care 2020; 24(1):80. doi: 10.1186/s13054-020-2770-5 [Crossref] [ Google Scholar]
- Chen L, Hong L, Ma A, Chen Y, Xiao Y, Jiang F. Intraoperative venous congestion rather than hypotension is associated with acute adverse kidney events after cardiac surgery: a retrospective cohort study. Br J Anaesth 2022; 128(5):785-95. doi: 10.1016/j.bja.2022.01.032 [Crossref] [ Google Scholar]
- Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009; 53(7):582-8. doi: 10.1016/j.jacc.2008.08.080 [Crossref] [ Google Scholar]
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005; 8(1):19-32. doi: 10.1080/1364557032000119616 [Crossref] [ Google Scholar]
- McGowan J, Straus S, Moher D, Langlois EV, O’Brien KK, Horsley T. Reporting scoping reviews-PRISMA ScR extension. J Clin Epidemiol 2020; 123:177-9. doi: 10.1016/j.jclinepi.2020.03.016 [Crossref] [ Google Scholar]
- Gordon M, Daniel M, Ajiboye A, Uraiby H, Xu NY, Bartlett R. A scoping review of artificial intelligence in medical education: BEME Guide No 84. Med Teach 2024; 46(4):446-70. doi: 10.1080/0142159x.2024.2314198 [Crossref] [ Google Scholar]
- Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 2018; 18(1):143. doi: 10.1186/s12874-018-0611-x [Crossref] [ Google Scholar]
- Neaton K, Voldanova L, Kiely T, Nagle C. Non-pharmacological treatments for shivering post neuraxial anaesthesia for caesarean section: a scoping review. Contemp Nurse 2024; 60(1):42-53. doi: 10.1080/10376178.2024.2310256 [Crossref] [ Google Scholar]
- Demirjian S, Bakaeen F, Tang WH, Donaldson C, Taliercio J, Huml A. Hemodynamic determinants of cardiac surgery-associated acute kidney injury. Crit Care Explor 2024; 6(4):e1063. doi: 10.1097/cce.0000000000001063 [Crossref] [ Google Scholar]
- Dang PT, Lopez BE, Togashi K. A decrease in effective renal perfusion pressure is associated with increased acute kidney injury in patients undergoing cardiac surgery. Cureus 2023; 15(9):e45036. doi: 10.7759/cureus.45036 [Crossref] [ Google Scholar]
- Alhulaibi AA, Alruwaili AM, Alotaibi AS, Alshakhs FN, Alramadhan HS, Koudieh MS. Validation of various prediction scores for cardiac surgery-associated acute kidney injury. J Saudi Heart Assoc 2022; 34(4):222-31. doi: 10.37616/2212-5043.1322 [Crossref] [ Google Scholar]
- Tohi Y, Takei Y, Nochioka K, Toyama H, Yamauchi M. Worsening right ventricular function during cardiac surgery is a strong predictor of postoperative acute kidney injury: a prospective observational study. Tohoku J Exp Med 2022; 258(2):129-41. doi: 10.1620/tjem.2022.J064 [Crossref] [ Google Scholar]
- Neuman J, Schulz L, Aneman A. Associations between mean systemic filling pressure and acute kidney injury: an observational cohort study following cardiac surgery. Acta Anaesthesiol Scand 2021; 65(3):373-80. doi: 10.1111/aas.13732 [Crossref] [ Google Scholar]
- Lopez MG, Shotwell MS, Morse J, Liang Y, Wanderer JP, Absi TS. Intraoperative venous congestion and acute kidney injury in cardiac surgery: an observational cohort study. Br J Anaesth 2021; 126(3):599-607. doi: 10.1016/j.bja.2020.12.028 [Crossref] [ Google Scholar]
- Kotani Y, Yoshida T, Kumasawa J, Kamei J, Taguchi A, Kido K. The impact of relative hypotension on acute kidney injury progression after cardiac surgery: a multicenter retrospective cohort study. Ann Intensive Care 2021; 11(1):178. doi: 10.1186/s13613-021-00969-4 [Crossref] [ Google Scholar]
- Farghaly A, Fahmy A, Ameen M, Taema KM, Hamed G. Blood pressure and blood pressure deficits as predictors of acute kidney injury in vasopressor dependent patients post cardiovascular surgery. Open Access Maced J Med Sci 2020; 8(B):542-7. doi: 10.3889/oamjms.2020.4357 [Crossref] [ Google Scholar]
- Hu R, Kalam Y, Broad J, Ho T, Parker F, Lee M. Decreased mean perfusion pressure as an independent predictor of acute kidney injury after cardiac surgery. Heart Vessels 2020; 35(8):1154-63. doi: 10.1007/s00380-020-01578-0 [Crossref] [ Google Scholar]
- Jin J, Yu J, Chang SC, Xu J, Xu S, Jiang W. Postoperative diastolic perfusion pressure is associated with the development of acute kidney injury in patients after cardiac surgery: a retrospective analysis. BMC Nephrol 2019; 20(1):458. doi: 10.1186/s12882-019-1632-3 [Crossref] [ Google Scholar]
- Che M, Wang X, Liu S, Xie B, Xue S, Yan Y. A clinical score to predict severe acute kidney injury in Chinese patients after cardiac surgery. Nephron 2019; 142(4):291-300. doi: 10.1159/000499345 [Crossref] [ Google Scholar]
- Jiang W, Shen B, Wang Y, Xu J, Luo Z, Ding X. Potentially modifiable predictors for renal replacement therapy in patients with cardiac surgery associated-acute kidney injury: a propensity score-matched case-control study. Braz J Cardiovasc Surg 2019; 34(1):33-40. doi: 10.21470/1678-9741-2018-0206 [Crossref] [ Google Scholar]
- Beaubien-Souligny W, Benkreira A, Robillard P, Bouabdallaoui N, Chassé M, Desjardins G. Alterations in portal vein flow and intrarenal venous flow are associated with acute kidney injury after cardiac surgery: a prospective observational cohort study. J Am Heart Assoc 2018; 7(19):e009961. doi: 10.1161/jaha.118.009961 [Crossref] [ Google Scholar]
- Jiang W, Xu J, Shen B, Wang C, Teng J, Ding X. Validation of four prediction scores for cardiac surgery-associated acute kidney injury in Chinese patients. Braz J Cardiovasc Surg 2017; 32(6):481-6. doi: 10.21470/1678-9741-2017-0116 [Crossref] [ Google Scholar]
- Ortega-Loubon C, Fernández-Molina M, Carrascal-Hinojal Y, Fulquet-Carreras E. Cardiac surgery-associated acute kidney injury. Ann Card Anaesth 2016; 19(4):687-98. doi: 10.4103/0971-9784.191578 [Crossref] [ Google Scholar]
- Xiao W, Liu W, Zhang J, Huang L, Liu Y, Hu J. Early persistent exposure to high CVP is associated with increased mortality and AKI in septic shock: a retrospective study. Am J Emerg Med 2023; 74:146-51. doi: 10.1016/j.ajem.2023.09.043 [Crossref] [ Google Scholar]
- Prakash J, Rao NS, Kumar S, Raghwendra KH, Saran K, Reddy SD. Study of relationship between central venous pressure and peripheral venous pressure during intraoperative period in neurosurgical patients. J Neuroanaesth Crit Care 2018; 5(1):15-20. doi: 10.1055/s-0037-1618328 [Crossref] [ Google Scholar]
- Wu J, Li J, Chen H, Shang X, Yu R. Optimization of central venous pressure during the perioperative period is associated with improved prognosis of high-risk operation patients. J Intensive Med 2023; 3(2):165-70. doi: 10.1016/j.jointm.2022.06.003 [Crossref] [ Google Scholar]