Arch Iran Med. 28(10):557-567.
doi: 10.34172/aim.34630
Original Article
Efficacy and Safety Analysis of Triple Therapy (Pabolizumab+Cryoablation+Renvastinib) for Patients with Unresectable Hepatocellular Carcinoma (uHCC)
Juan Lei Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Writing – original draft, 1 
Zhonghua Chen Conceptualization, Funding acquisition, Project administration, Supervision, Visualization, Writing – review & editing, 2, *
Author information:
1Medical Service Training Center, 900th Hospital of Joint Logistics Support Force, Fuzhou, China
2Department of Radiotherapy Oncology, 900th Hospital of Joint Logistics Support Force, Fuzhou, China
Abstract
Background:
To determine whether employing a monoclonal antibody against programmed death receptor-1 (PD-1) improves the safety and effectiveness of cryoablation used with Renvastinib to treat unresectable hepatocellular carcinoma (uHCC).
Methods:
Our study retrospectively enrolled 232 uHCC patients who were treated at our medical center between January 2019 and December 2023. Propensity score matching (PSM) was employed in this study for 1:1 matching, and 86 patients were matched in each group. Following matching, the two groups’ negative events, and assessments were made on the objective response rate (ORR), disease control rate (DCR), progression-free survival (PFS), and overall survival (OS). When comparing two groups, a group t test was employed to determine whether the quantitative data were normally distributed. The two groups’ survival rates were calculated using the Kaplan-Meier method, survival curves were made, and the log-rank test was performed to find differences between the two groups.
Results:
The median follow-up period was 28 months. Forty deaths (46.0%) happened in the double group, whereas 33 deaths (38.0%) occurred in the triple group. The ORR and DCR of the triple treatment group were significantly higher than those of the double therapy group (ORR: 35.6% vs. 14.5%, P=0.08; DCR: P=0.003; 86.1% vs. 64.1%). Compared to the double group, the OS and PFS rates in the triple group were considerably higher (P=0.045 and P=0.026, respectively). Analysis of univariate and multivariable Cox risk proportional models showed that AFP level (HR=2.37, P=0.001) and treatment regimen (HR=0.60, P=0.38) were independent risk factors for OS. Independent risk variables for PFS included diabetes mellitus (HR=1.94, P=0.05), prior local treatment (HR=0.63, P=0.014), treatment protocol (HR=0.65, P=0.025), and distant metastasis (HR=0.58, P=0.09). The incidence of negative reactions did not differ significantly between the two groups (P>0.05).
Conclusion:
Compared with cryoablation combined with renvatinib, cryoablation combined with renvatinib and PD-1 mAb significantly improved the efficacy and survival of patients with uHCC without increasing adverse events, giving unresectable liver cancer a clinical foundation for treatment optimization.
Keywords: Cryoablation, Immunotherapy, Renvastinib, Triple therapy, Unresectable hepatocellular carcinoma
Copyright and License Information
© 2025 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Lei J, Chen Z. Efficacy and safety analysis of triple therapy (pabolizumab+cryoablation+renvastinib) for patients with unresectable hepatocellular carcinoma (uHCC). Arch Iran Med. 2025;28(10):557-567. doi: 10.34172/aim.34630
Introduction
Hepatocellular carcinoma (HCC) ranks among the top causes of death among cirrhosis patients.1 However, only 15% of liver cancer patients receive radical treatment. Therefore, exploring treatment strategies for unresectable hepatocellular carcinoma (uHCC) is key to improving patient prognosis.2-4 Common local treatments include radiofrequency ablation, microwave ablation, cryoablation, and interventional therapy.5-7 Among these treatments, cryoablation has been increasingly used because of its advantages, such as minimal damage to large blood vessels, reduced risk of vascular complications, low incidence of pain and controllable formation of ice balls.8 Cryoablation can also produce “ectopic tumor suppression” so that local treatment and immunotherapy can achieve a more lasting effect, providing a theoretical basis for combining cryoablation with targeting and immunotherapy.9-11
In recent years, systemic therapies for liver cancer, such as sorafenib, Renvastinib and donafenib, have been recommended as first-line therapies for uHCC. The FDA has authorized attilizumab, a PD-L1 monoclonal antibody, for treatment of uHCC. Although targeted therapy and immunotherapy play important roles in controlling liver cancer progression, the objective response rate (ORR) is still less than 30%, and the ORR of the first-line treatment for HCC, bevacizumab combined with PD-L1 (T + A), is only 27%.12 Compared with treatment with targeted drugs alone, transhepatic arterial chemoembolization (TACE) combined with targeted drugs extends the median total survival (OS) and median progression-free survival (PFS) of patients (P < 0.05). Studies have also shown that immune checkpoint inhibitors combined with ablation therapy increase the median OS of patients with liver cancer (P < 0.05).13 It can be concluded that for uHCC patients, local ablation combined with targeted or immunodrug therapy can improve survival. In addition, local cryoablation, as an important local therapy, has the unique advantage of inducing a specific tumor immune response by releasing tumor-specific antigens.14,15 Therefore, immunotherapy on the basis of cryoablation therapy creates conditions for achieving a durable and enhanced antitumor immune response. Nevertheless, it is unknown if local cryoablation in conjunction with renvastinib and PD-1 monoclonal antibodies is safe and effective.
Materials and Methods
Research Subjects
This study included uHCC patients treated at our medical center from January 2019 to December 2023.
Inclusion criteria: (1) According to the American Academy of Hepatology’s practice guidelines, patients with uHCC who have been diagnosed by imaging (enhanced CT/MRI or pathological biopsy) and are undergoing cryoablation in conjunction with lenvatinib (double combination); (2) Child‒Pugh Grade A or B (score ≤ 7 points); (3) BCLC stage B or C; and (4) a physical condition score (ECOG PS) of 0~1.
Exclusion criteria: (1) Having hepatic metastases or cholangiocarcinoma; (2) A treatment cycle of lenvatinib of less than 1 month; (3) Less than 4 PD-1 monoclonal antibodies; (4) Severe comorbidities, including severe heart, lung, kidney or coagulation dysfunction and other uncontrolled chronic diseases and mental disorders; (5) HIV infection; (6) Pregnant women or children; (7) Incomplete clinical data (Figure 1).
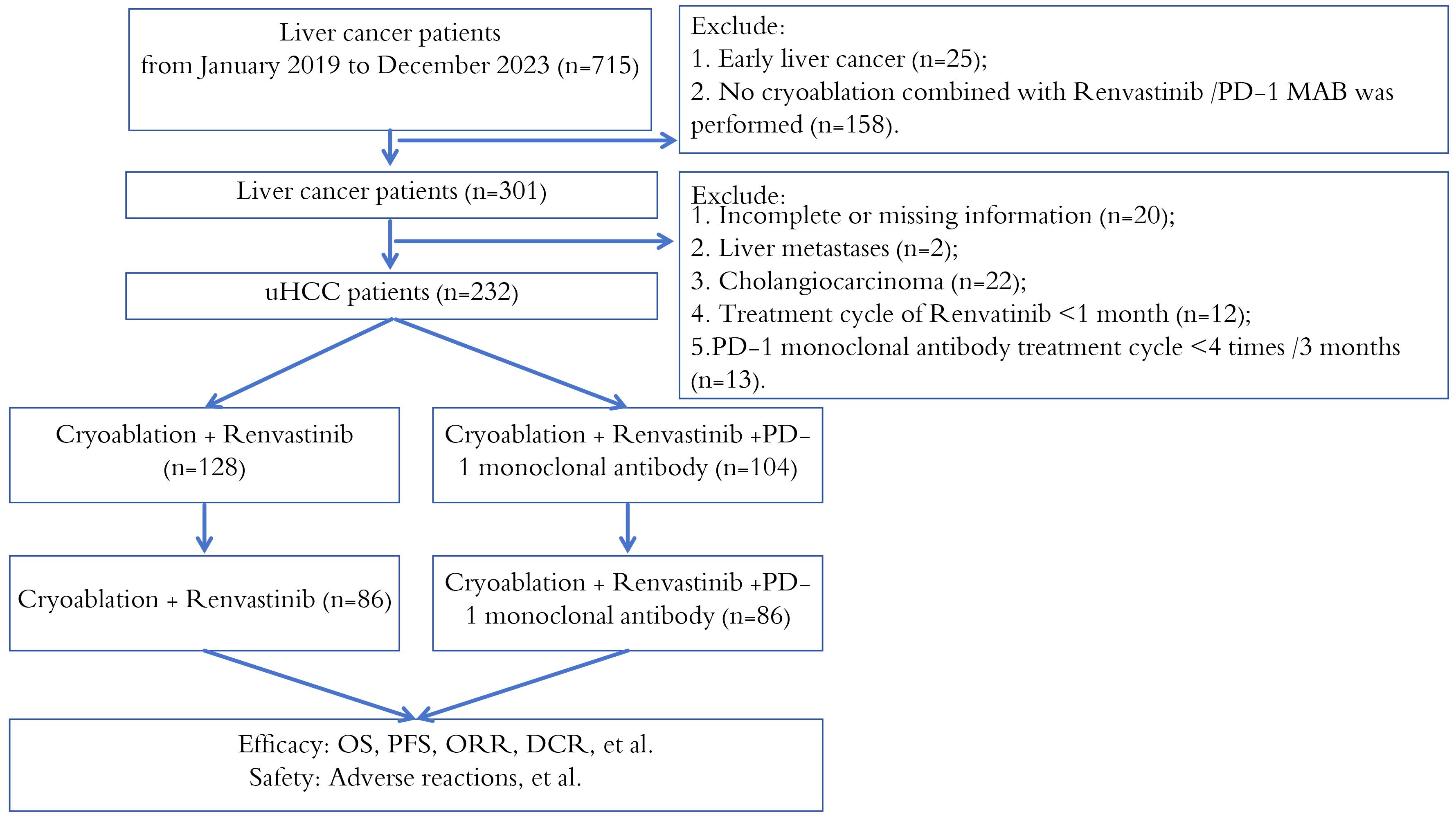
Figure 1.
Patient Enrollment Flow Chart
.
Patient Enrollment Flow Chart
Research Methods
Cryoablation procedure: Using a cryo-probe guided by CT and the cryo-care system (Endocare), a twofold freezing-thawing cycle was performed. The double freeze‒thaw cycle consisted of 20 minutes of freezing, followed by 10 minutes of thawing and 15 minutes of freezing, and the freezing probe temperature was reduced to -165 ± 2 °C within 1 minute. To prevent the ablation from spreading to nearby vital structures, real-time ultrasound monitoring of the ablation procedure was undertaken. The hemostatic gelatin sponge was inserted into the sheath, the hemostatic sponge was plugged, and the sheath was removed.
Depending on body mass. PD-1 monoclonal antibody (200 mg) was intravenously administered once every 3 weeks, and the drug dose was adjusted according to the manufacturer’s instructions. The revised Solid Tumor Response Assessment Criteria (mRECIST) were used every 8-12 weeks to assess patient response to therapy.
Curative Effect Evaluation
OS is defined as the period of time from the beginning of treatment and the last follow-up or death (for any reason). PFS is defined as the interval between the initiation of treatment and the tumor’s progression (in any manner), death (for any cause), or the most recent follow-up, whichever came first.
Complete response (CR), partial response (PR), stable disease (SD), progressive disease (PD), objective response rate (ORR), and disease control rate (DCR) were among the mRECIST criteria used to evaluate efficacy.
Safety Evaluation
CTCAE version 5.0 was used to analyze adverse events. Level 1: Mild; asymptomatic or mild; clinical or diagnostic findings only; no treatment needed. Level 2: Moderate; requiring minor, local or noninvasive treatment; Age-appropriate restriction of instrumental activities of daily living. Level 3: Severe or medically significant but not immediately life-threatening; leading to hospitalization or extended hospitalization; being incapacitated; and limiting one’s ability to undertake self-rational daily living activities. Level 4: Potentially fatal; immediate medical care is required. Level 5: Death as a result of an adverse incident.
Follow-up Visit
The last follow-up ended on March 31, 2024, and the efficacy follow-up was regularly performed every 3 months after the initial treatment. Thorough medical history and physical examination were part of every follow-up, as well as hematological and biochemical tests, enhanced abdominal CT or MRI, chest CT and other imaging tests, and laboratory tests, including PLT, liver function, AFP, etc. During follow-up, treatment could be discontinued if there was an intolerable toxic reaction, tumor progression, or a change in the treatment plan. On the basis of the results of the multidisciplinary panel discussion and the requirements of the patient, the choice of subsequent treatment, such as second-line targeted agents, PD-1 inhibitors (for patients receiving dual therapy), radiotherapy (including 125I particle brachytherapy), TACE, hepatic arterial infusion chemotherapy (HAIC), or optimal supportive treatment, was determined.
Statistical Analysis
SPSS 26, GraphPad Prism 9 and R 4.0 were used for data analysis. To avoid selection bias in retrospective cohort studies, propensity score matching (PSM) (0.2 of the SD of the logit of the PS)16 was used. By using the logit model, factors that may affect treatment efficacy were identified, including ECOG status, age, sex, BMI, disease etiology, baseline liver function, degree of portal vein cancer thrombus, baseline AFP level, previous treatment, BCLC grade, Child grade, portal hypertension, and the presence or absence of distant metastasis.
The minimum fully confounding variable set was identified and selected through a causal directed acyclic graph (cDAG) to ensure the adjustment of all potential confounding factors. Normally distributed quantitative data are represented as mean ± SD. The balance of confounding factors in the matched population should be evaluated using the standardized mean difference (SMD) (SMD < 0.1).17
Results
Analysis of Clinical Medical Records
In total 232 patients were part of the PSM analysis, and after matching, 172 comparable HCC patients (1:1 matching) were selected for analysis, including 86 patients in either the triple and double groups (Figure 1). After matching, the difference between the two groups was reduced, and the factors included in the analysis were balanced in both groups (P value > 0.05). In the overall cohort after PSM, the proportion of patients < 60 years old was greater than that of patients ≥ 60 years old, and the proportion of men was higher. A total of 157 patients (91.2%) were infected with HBV alone, 93.0% and 89.5% were in the triple group and the double group, respectively, and only 2 patients had no history of cirrhosis. Most of the enrolled patients had multiple lesions, including 74 patients (86%) with triple combination and 69 patients (80.2%) with double combination. Most of the patients had vascular invasion, including 55 patients (64.0%) with triple combination and 58 patients (67.4%) with double combination. There were 34 patients (39.5%) and 28 patients (32.6%) with distant metastasis in the two groups (double and triple). There were 124 patients (73%) with stage C BCLC, 60 patients (69.8%) in the triple group and 64 patients (74.4%) in the double group. Most of the patients had Child‒Pugh stage A disease, including 55 patients (64.0%) in the triple group and 60 patients (69.8%) in the double group. Following matching, the majority of patients had already undergone cancer-related treatment (Table 1).
Table 1.
Clinical Features before and after PSM in the Cryo + Lenvatinib + anti-PD-1 Group and Cryo + Lenvatinib Group
|
Project
|
Before PSM
|
After PSM
|
|
Total (n=232)
|
Triple (n=104)
|
Double (n=128)
|
Statistical value
|
P
value
|
Triple (n=86)
|
Double (n=86)
|
Statistical value
|
P
value
|
| Gender [ (%)] |
|
|
|
χ2 = 0.000 |
0.987 |
|
|
χ2 = 0.657 |
0.418 |
| Female |
20 (8.6) |
9 (8.7) |
11 (8.6) |
|
|
9 (10.5) |
6 (7.0) |
|
|
| Male |
212 (91.4) |
95 (91.3 |
117 (91.4 |
|
|
77 (89.5) |
80 (93.0 |
|
|
| Age [ (%)] |
|
|
|
χ2 = 0.100 |
0.752 |
|
|
χ2 = 0.102 |
0.749 |
| < 60 years old |
152 (65.5) |
67 (64.4) |
85 (66.4) |
|
|
55 (64.0) |
57 (66.3) |
|
|
| ≥ 60 years old |
80 (34.5) |
37 (35.6 |
43 (33.6) |
|
|
31 (36.0) |
29 (33.7) |
|
|
| BMI [ (%)] |
|
|
|
χ2 = 0.525 |
0.469 |
|
|
χ2 = 0.024 |
0.878 |
| < 24 kg/m2 |
102 (44.0) |
43 (41.3) |
59 (46.1) |
|
|
37 (43.0) |
38 (44.2) |
|
|
| ≥ 24 kg/m2 |
130 (56.0) |
61 (58.7) |
69 (53.9) |
|
|
49 (57.0) |
48 (55.8) |
|
|
| Portal hypertension [ (%)] |
χ2 = 0.009 |
0.926 |
|
|
χ2 = 0.000 |
> 0.05 |
| Yes |
188 (81.0) |
84 (80.8) |
104 (81.2) |
|
|
70 (81.4) |
70 (81.4) |
|
|
| No |
44 (19.0) |
20 (19.2) |
24 (18.8) |
|
|
16 (18.6) |
16 (18.6) |
|
|
| Etiology [ (%)] |
χ2 = 3.561 |
0.169 |
|
|
χ2 = 0.657 |
0.72 |
| HBV |
206 (88.8) |
96 (92.3 |
110 (85.9) |
|
|
80 (93.0) |
77 (89.5) |
|
|
| HCV |
13 (5.6) |
2 (1.9) |
9 (7.0) |
|
|
2 (2.3) |
3 (3.5) |
|
|
| Other |
19 (8.2) |
6 (5.8) |
9 (7.0) |
|
|
4 (4.7) |
6 (7.0) |
|
|
| Antivirus [ (%)] |
χ2 = 2.740 |
0.098 |
|
|
χ2 = 1.758 |
0.185 |
| Yes |
190 (81.9) |
90 (86.5) |
100 (78.1) |
|
|
72 (83.7) |
65 (75.6) |
|
|
| No |
42 (18.1) |
14 (13.5) |
28 (21.9) |
|
|
14 (16.3) |
21 (24.4) |
|
|
| AFP [ (%)] |
χ2 = 9.316 |
0.002 |
|
|
χ2 = 0.595 |
0.440 |
| < 400 ng/mL |
126 (54.3) |
68 (65.4) |
58 (45.3) |
|
|
52 (60.5) |
47 (54.7) |
|
|
| 2400 ng/mL |
106 (45.7) |
36 (34.6) |
70 (54.7) |
|
|
34 (39.5) |
39 (45.3) |
|
|
| PLT ( × 109/L) |
125 (90.0~187.0) |
118 (80.0146.0) |
142 (96.2~203.8) |
U = 5183 0.002 |
0.002 |
119.5 (88.8~155.8) |
133 (92.8~203.3) |
U = 3180 |
0.115 |
| ALT (U/I) |
35 (22.0~57.0) |
37 (24.0~74.5) |
33 (19.5~53.1) |
U = 5826 0.121 |
0.121 |
36 (23.5~55.3) |
33.5 (21.8~59.0) |
U = 3530 |
0.607 |
| AST (U/L) |
41 (28.0~77.9) |
38 (27.3~78.8) |
44 (28.3~77.5) |
U = 6583 0.747 |
0.747 |
37 (27.0~61.2) |
37 (27.0~76.3) |
U = 3655 |
0.896 |
| TBil (μmal/L) |
17.5 (12.5~23.6) |
18.1 (11.4~25.6) |
17.0 (12.8~22.8) |
U = 6284 |
0.702 |
18 (11.4~25.6) |
16.9 (12.3~22.5) |
U = 3424 |
0.401 |
| Child‒Pugh grading [(%)] |
χ2 = 0.323 |
0.57 |
|
|
χ2 = 0.656 |
0.418 |
| A-level |
154 (66.4 |
67 (64.4) |
87 (68.0) |
|
|
55 (64.0) |
60 (69.8) |
|
|
| B-level |
78 (33.6) |
3 (35.6) |
41 (32.0) |
|
|
31 (36.0) |
26 (30.2) |
|
|
| ALBI grading [(%)] |
χ2 = 1.039 |
0.595 |
|
|
χ2 = 0.089 |
0.502 |
| Level 1 |
49 (21.1) |
19 (18.3 |
30 (23.4) |
|
|
17 (19.8) |
22 (25.6) |
|
|
| Level 2 |
171 (73.7) |
80 (76.9) |
91 (71.1) |
|
|
65 (75.6) |
62 (72.1) |
|
|
| Level 3 |
12 (5.2) |
5 (4.8) |
7 (5.5) |
|
|
4 (4.7) |
2 (2.3) |
|
|
| Number of tumors [(%)] |
χ2 = 4.247 |
0.039 |
|
|
χ2 = 1.037 |
0.309 |
| Single |
45 (19.4 |
14 (13.5) |
31 (24.2) |
|
|
12 (14.0) |
17 (19.8) |
|
|
| Multiple |
187 (80.6) |
90 (86.5) |
97 (75.8) |
|
|
74 (86.0) |
69 (80.2) |
|
|
| Maximum diameter of tumor [(%)] |
χ2 = 10.918 |
0.001 |
|
|
χ2 = 0.611 |
0.434 |
| < 7.07 cm |
133 (57.3) |
72 (69.2) |
61 (47.7 |
|
|
55 (64.0) |
50 (58.1) |
|
|
| ≥ 7.07 cm |
99 (42.7) |
32 (30.8 |
67 (52.3) |
|
|
31 (36.0) |
36 (41.9) |
|
|
| Vascular invasion [(%)] |
χ2 = 0.998 |
0.318 |
|
|
χ2 = 0.232 |
0.630 |
| Yes |
153 (65.9) |
65 (62.5) |
88 (68.8) |
|
|
55 (64.0) |
58 (67.4) |
|
|
| No |
79 (34.1) |
39 (37.5) |
40 (31.2) |
|
|
31 (36.0) |
28 (32.6) |
|
|
| Distant metastasis [(%)] |
χ2 = 0.353 |
0.553 |
|
|
χ2 = 0.908 |
0.341 |
| Yes |
80 (34.5) |
38 (36.5 |
42 (32.8) |
|
|
34 (39.5) |
28 (32.6) |
|
|
| No |
152 (65.5) |
66 (63.5) |
85 (66.4) |
52 (60.5) |
57 (66.3) |
52 (60.5) |
57 (66.3) |
|
|
| BCIC grading [(%)] |
χ2 = 1.041 |
0.308 |
|
|
χ2 = 0.497 |
0.497 |
| B-level |
68 (29.3 |
34 (32.7) |
34 (26.6) |
|
|
26 (30.2) |
22 (25.6) |
|
|
| C-level |
164 (70.7) |
70 (67.3) |
94 (73.4) |
|
|
60 (69.8) |
64 (74.4) |
|
|
| Diabetes [(%)] |
|
|
|
χ2 = 1.252 |
0.263 |
|
|
χ2 = 0.154 |
0.695 |
| Yes |
46 (19.8 |
24 (23.1) |
22 (17.2) |
|
|
17 (19.8) |
15 (17.4) |
|
|
| No |
186 (80.2) |
80 (76.9) |
106 (82.8) |
|
|
69 (80.2) |
71 (82.6) |
|
|
| Liver cirrhosis [(%)] |
χ2 = 0.170 |
0.009 |
|
|
χ2 = 2.024 |
0.155 |
| Yes |
224 (96.6) |
104 (100.0) |
120 (93.8) |
|
|
86 (100.0 |
84 (97.7) |
|
|
| No |
8 (3.4) |
0 (0.0) |
8 (6.2) |
|
|
0 (0.0) |
2 (2.3) |
|
|
| ECOGPS score [(%)] |
χ2 = 0.816 |
0.366 |
|
|
χ2 = 0.821 |
0.312 |
| 0 |
1 (0.4) |
0 (0.0) |
1 (0.8) |
|
|
0 (0.0) |
0 (0.0) |
|
|
| 1 |
231 (99.6) |
104 (100.0) |
127 (99.2) |
|
|
86 (100.0) |
86 (100.0) |
|
|
| Previous local treatment [(%)] |
χ2 = 7.118 |
0.008 |
|
|
χ2 = 0.841 |
0.359 |
| Yes |
118 (50.9) |
63 (60.6) |
55 (43.0) |
|
|
49 (57.0) |
43 (50.0) |
|
|
| No |
114 (49.1) |
41 (39.4) |
73 (57.0) |
|
|
37 (43.0) |
43 (50.0) |
|
|
| Previous systematic treatment [(%)] |
χ2 = 0.704 |
0.401 |
|
|
χ2 = 0.073 |
0.787 |
| Yes |
22 (9.5) |
8 (7.7) |
14 (10.9) |
|
|
7 (8.1) |
8 (9.3) |
|
|
| No |
210 (90.5) |
96 (92.3) |
114 (89.1) |
|
|
79 (91.9) |
78 (90.7) |
|
|
| Cryoablation [(%)] |
χ2 = 0.000 |
0.984 |
|
|
χ2 = 0.462 |
0.497 |
| 1 |
69 (29.7) |
31 (29.8) |
38 (29.7) |
|
|
26 (30.2) |
22 (25.6) |
|
|
| > 1 |
163 (70.3) |
73 (70.2) |
90 (70.3) |
|
|
60 (69.8) |
64 (74.4) |
|
|
Comparison of OS and PFS between the Two Groups
There were 40 deaths (46.0%) in the double group and 33 deaths (38%) in the triple group with a median follow-up of 28 months. The survival rate was considerably greater for patients in the triple group than for those in the double group. The OS and PFS of patients in the triple group were 34.6 months and 8.0 months. The OS and PFS in the double group were 19.0 months and 6.0 months. The OS and PFS of the two groups differed statistically significantly (P values: 0.045 and 0.026, respectively) (Figure 2).
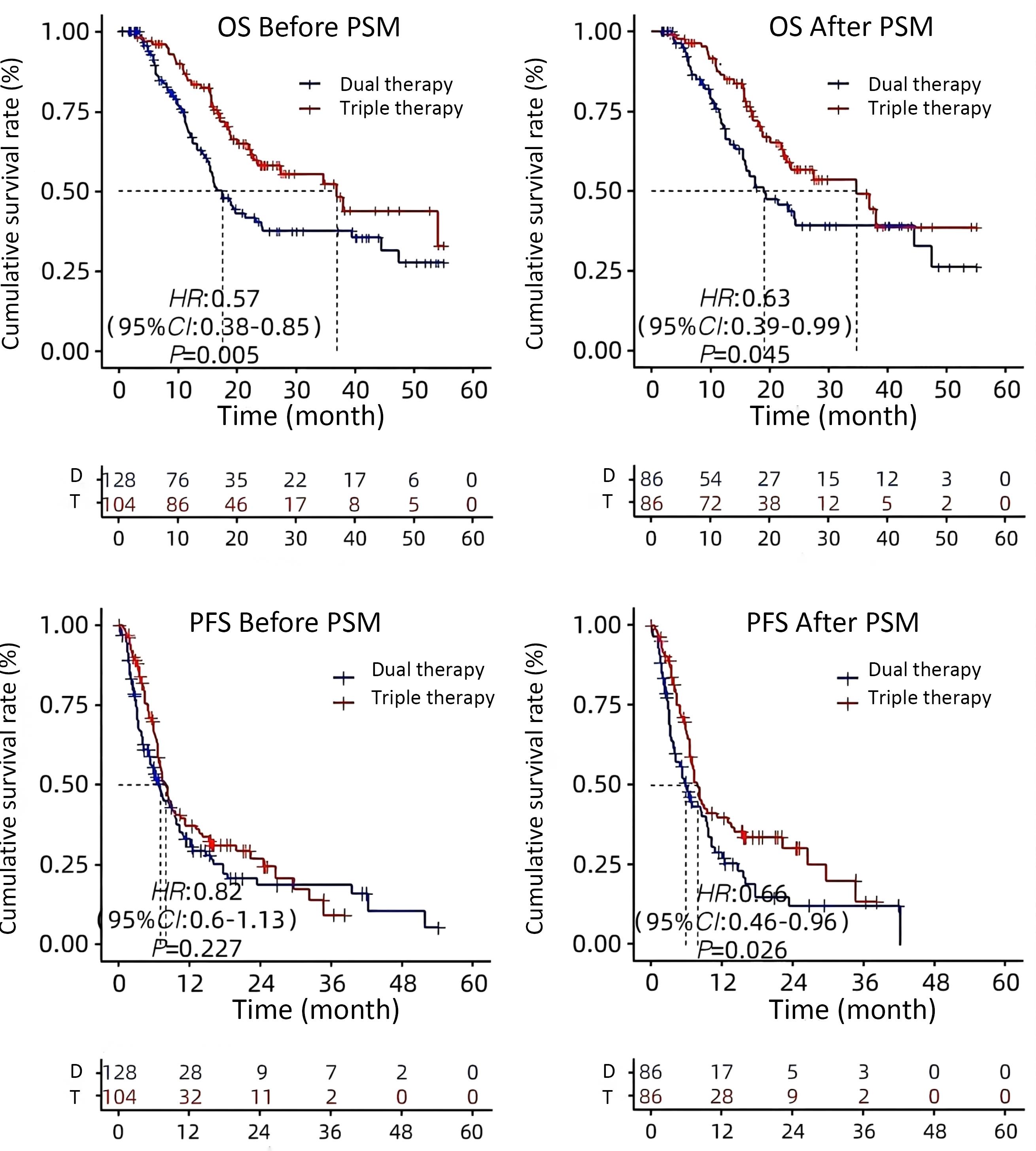
Figure 2.
OS and PFS Comparisons before and after PSM
.
OS and PFS Comparisons before and after PSM
Cox Regression Analysis after PSM
The treatment regimen and AFP level were found to be independent factors affecting OS (P < 0.05). PFS was observed to be independently influenced by treatment regimen, diabetes mellitus status, prior local treatment, and distant metastasis (all P < 0.05) (Table 2). Cox regression analysis before PSM revealed that treatment regimen, AFP level, previous local treatment, and number of cryoablations were independent factors influencing OS (P < 0.05) (Table 3). Cox regression analysis before and after PSM revealed that the treatment regimen and AFP level were independent influencing factors for OS.
Table 2.
Single Factor Regression Analysis of Factors Influencing OS and PFS after PSM
|
Item
|
OS
|
PFS
|
|
Univariate analysis
|
Multivariate analysis
|
Univariate analysis
|
Multivariate analysis
|
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
| Treatment plan (triple vs double) |
0.63(0.39~0.99) |
0.047 |
0.6(0.37~0.97) |
0.038 |
0.66(0.46~0.96) |
0.028 |
0.65 (0.44~0.95) |
0.025 |
| Gender (male vs female) |
0.73(0.31~1.68) |
0.453 |
|
|
1.09(0.60~1.98) |
0.782 |
|
|
| Age ( > 60 years vs < 60 years) |
0.88(0.54~1.43) |
0.615 |
|
|
1.03(0.70~1.51) |
0.886 |
|
|
| BMI ( ≥ 24ky/m2 vs < 24 kg/m2) |
1.49(0.93~2.39) |
0.100 |
|
|
1.37(0.94~2.00) |
0.099 |
|
|
| Child‒Pugh grading (B vs. A) |
0.95(0.58~1.57) |
0.842 |
|
|
0.96(0.65~1.42) |
0.847 |
|
|
| BCLC grading (C and B) |
1.82(1.05~3.14) |
0.032 |
0.86(0.33~2.23) |
0.758 |
0.79(0.54~1.17) |
0.234 |
|
|
| Diabetes (Yes or No) |
0.7(0.37~1.30) |
0.256 |
|
|
1.69(1.08~2.64) |
0.022 |
1.94(1.22~3.09) |
0.005 |
| Portal hypertension (Yes or No) |
2.08(1.03~4.20) |
0.042 |
1.73(0.83~3.58) |
0.142 |
0.89(0.57~1.41) |
0.625 |
|
|
| Cirrhosis (Yes or No) |
20.72(0.01~5207.00) |
0.448 |
|
|
0.81(0.20~3.27) |
0.763 |
|
|
| HBV (Yes or No) |
0.89(0.38~2.05) |
0.776 |
|
|
0.88(0.45~1.75) |
0.722 |
|
|
| Antiviral (Yes or No) |
0.93(0.52~1.63) |
0.789 |
|
|
0.94(0.59~1.48) |
0.779 |
|
|
| Number of tumors ( > 1 vs 1) |
0.96(0.54~1.73) |
0.901 |
|
|
1(0.61~1.62) |
0.988 |
|
|
| Tumor size ( ≥ 7.07 cm vs < 7.07 cm) |
1.68(1.05~2.68) |
0.030 |
1.18(0.70~1.98) |
0.537 |
0.76(0.52~1.12) |
0.16 |
|
|
| AFP ( > 400 ng/mL vs < 400 ng/mL) |
2.46(1.55~3.92) |
≤ 0.001 |
2.37(1.44~3.88) |
0.001 |
1.06(0.73~1.53) |
0.772 |
|
|
| Previous local treatment (Yes or No) |
0.55(0.34~0.87) |
0.012 |
0.67(0.41~1.11) |
0.123 |
0.63(0.44~0.91) |
0.013 |
0.63(0.43~0.89) |
0.014 |
| Previous systematic treatment (Yes or No) |
0.64(0.26~1.58) |
0.331 |
|
|
0.74(0.39~1.42) |
0.372 |
|
|
| Follow up local treatment (Yes or No) |
0.41(0.10~1.70) |
0.220 |
|
|
1.8(0.87~3.72) |
0.110 |
|
|
| Subsequent systematic treatment (Yes or No) |
0.39(0.16~0.97) |
0.042 |
0.62(0.24~1.61) |
0.325 |
1.17(0.72~1.89) |
0.532 |
|
|
| Cryoablation frequency ( > 1 vs 1) |
0.79(0.47~1.33) |
0.382 |
|
|
1.56(0.99~2.45) |
0.054 |
|
|
| Distant metastasis (Yes or No) |
1.16(0.72~1.86) |
0.539 |
|
|
0.53(0.35~0.80) |
0.002 |
0.58 (0.38~0.87) |
0.009 |
| Vascular invasion (Yes or No) |
1.86(1.11~3.12) |
0.019 |
1.79(0.73~4.41) |
0.204 |
0.89(0.61~1.30) |
0.553 |
|
|
Table 3.
Multifactor Regression Analysis of Factors Influencing OS and PFS before PSM
|
Project
|
OS
|
PFS
|
|
Univariate analysis
|
Multivariate analysis
|
Univariate analysis
|
Multivariate analysis
|
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
HR (95% CI)
|
P
|
| Treatment plan (triple vs double) |
0.57(0.38~0.85) |
0.005 |
0.63(0.41~0.98) |
0.039 |
0.82(0.60~1.13) |
0.228 |
0.77(0.54~1.10) |
0.149 |
| Gender (male vs female) |
0.86(0.42~1.78) |
0.693 |
|
|
1.19(0.70~2.02) |
0.526 |
|
|
| Age (260 years vs. < 60 years) |
0.83(0.55~1.26) |
0.379 |
|
|
0.9(0.64~1.25) |
0.520 |
|
|
| BMI ( ≥ 24 kg/m2 vs < 24 kg/m2) |
1.31(0.88~1.96) |
0.179 |
|
|
1.24(0.90~1.70) |
0.190 |
|
|
| Child‒Pugh grading (B vs. A) |
1.22(0.81~1.84) |
0.335 |
|
|
0.99(0.71~1.38) |
0.946 |
|
|
| BC LC classification(C vs. B) |
1.69(1.07~2.65) |
0.024 |
0.92(0.41~2.07) |
0.846 |
0.79(0.57~1.10) |
0.171 |
0.61(0.32~1.16) |
0.132 |
| Diabetes (Yes or No) |
0.72(0.43~1.22) |
0.227 |
|
|
1.44(0.98~2.12) |
0.062 |
|
|
| Portal hypertension (Yes or No) |
1.72(0.99~3.00) |
0.053 |
|
|
0.89(0.60~1.31) |
0.549 |
|
|
| Cirrhosis (Yes or No) |
1.12(0.41~3.06) |
0.819 |
|
|
1.04(0.46~2.35) |
0.929 |
|
|
| HBV (Yes or No) |
1.08(0.56~2.07) |
0.826 |
|
|
0.97(0.58~1.60) |
0.894 |
|
|
| Antiviral (Yes or No) |
0.77(0.48~1.24) |
0.285 |
|
|
0.86(0.57~1.29) |
0.464 |
|
|
| Number of tumors ( > 1 vs 1) |
0.85(0.53~1.35) |
0.487 |
|
|
1.09(0.73~1.62) |
0.682 |
|
|
| Tumor size ( > 7.07 cm vs < 7.07 cm) |
1.83(1.24~2.71) |
0.002 |
1.09(0.71~1.68) |
0.689 |
0.76(0.55~1.05) |
0.100 |
0.71(0.49~1.02) |
0.064 |
| AFP ( ≥ 400 ng/mL vs < 400 ng/mL) |
2.11(1.42~3.12) |
< 0.001 |
1.75(1.16~2.64) |
0.008 |
0.94(0.69~1.29) |
0.709 |
1(0.72~1.40) |
0.989 |
| Previous local treatment (Yes or No) |
0.45(0.30~0.68) |
< 0.001 |
0.58(0.38~0.90) |
0.014 |
0.84(0.61~1.15) |
0.274 |
0.78(0.56~1.09) |
0.152 |
| Previous systematic treatment (Yes or No) |
0.67(0.32~1.37) |
0.270 |
|
|
0.91(0.55~1.50) |
0.701 |
|
|
| Follow up local treatment (Yes or No) |
0.26(0.06~1.08) |
0.064 |
|
|
1.63(0.88~3.01) |
0.120 |
|
|
| Subsequent systematic treatment (Yes or No) |
0.41(0.20~0.84) |
0.015 |
0.66(0.30~1.42) |
0.284 |
1.16(0.77~1.74) |
0.489 |
1.18(0.74~1.86) |
0.491 |
| Cryoablation frequency ( > 1 vs 1) |
0.62(0.41~0.95) |
0.028 |
0.6(0.39~0.93) |
0.023 |
1.43(0.97~2.10) |
0.070 |
1.35(0.91~2.00) |
0.135 |
| Distant metastasis (Yes or No) |
0.9(0.60~1.38) |
0.661 |
|
|
1.12(0.81~1.56) |
0.498 |
|
|
| Vascular invasion (Yes or No) |
1.79(1.15~2.76) |
0.009 |
1.73(0.78~3.82) |
0.178 |
0.9(0.65~1.25) |
0.523 |
1.42(0.74~2.71) |
0.292 |
Comparison of Tumor Response between the Two Groups
Compared to the double group, the triple group’s ORR (35.6% vs 14.5%) and DCR (86.1% vs 64.1%) were considerably higher (P = 0.08 and 0.0003, respectively). The triple group had lower PD (18.3% vs. 36.0%) and higher PR (25.6% vs. 11.6%) than the double group; these differences were statistically significant (P values were 0.0003 and 0.019, respectively) (Table 4).
Table 4.
Tumor Response
|
Evaluation of tumor efficacy
|
Before PSM
|
After PSM
|
|
Triple
|
Double
|
P
|
Triple
|
Double
|
P
|
| CR [(%)] |
9(8.7) |
5(3.9) |
0.131 |
7(8.1) |
4(4.7) |
0.350 |
| PR [(%)] |
27(26.0) |
13(10.2) |
0.002 |
22(25.6) |
10(11.6) |
0.019 |
| SD [(%)] |
50(48.1) |
66(51.6) |
0.597 |
43(50.0) |
41(47.7) |
0.760 |
| PD [(%)] |
18(17.3) |
44(34.4) |
0.003 |
14(18.3) |
31(36.0) |
0.003 |
| ORR [(%)] |
36(34.6) |
14(14.1) |
0.000 |
29(35.6) |
14(14.5) |
0.008 |
| DCR [(%)] |
86(82.7) |
84(65.6) |
0.003 |
72(86.1) |
55(64.1) |
0.003 |
Subgroup Analysis
The double group’s patient OS was extended by receiving more than one cryoablation (24.2 months vs. 12.6 months, P = 0.08) (Figure 3). The median overall survival (OS) for Child-Pugh grade A patients were considerably longer in the triple group than in the double group (36.97 months vs. 17.55 months, P = 0.034) (Figure 4). The median OS for patients with BCLC stages B and C did not change significantly between triple therapy and double therapy (P values were 0.198 and 0.133, respectively) (Figure 5). The triple group had a considerably longer median OS (34.6 months vs. 15.5 months, P = 0.048) than the double group for patients with distant metastases (Figure 6).
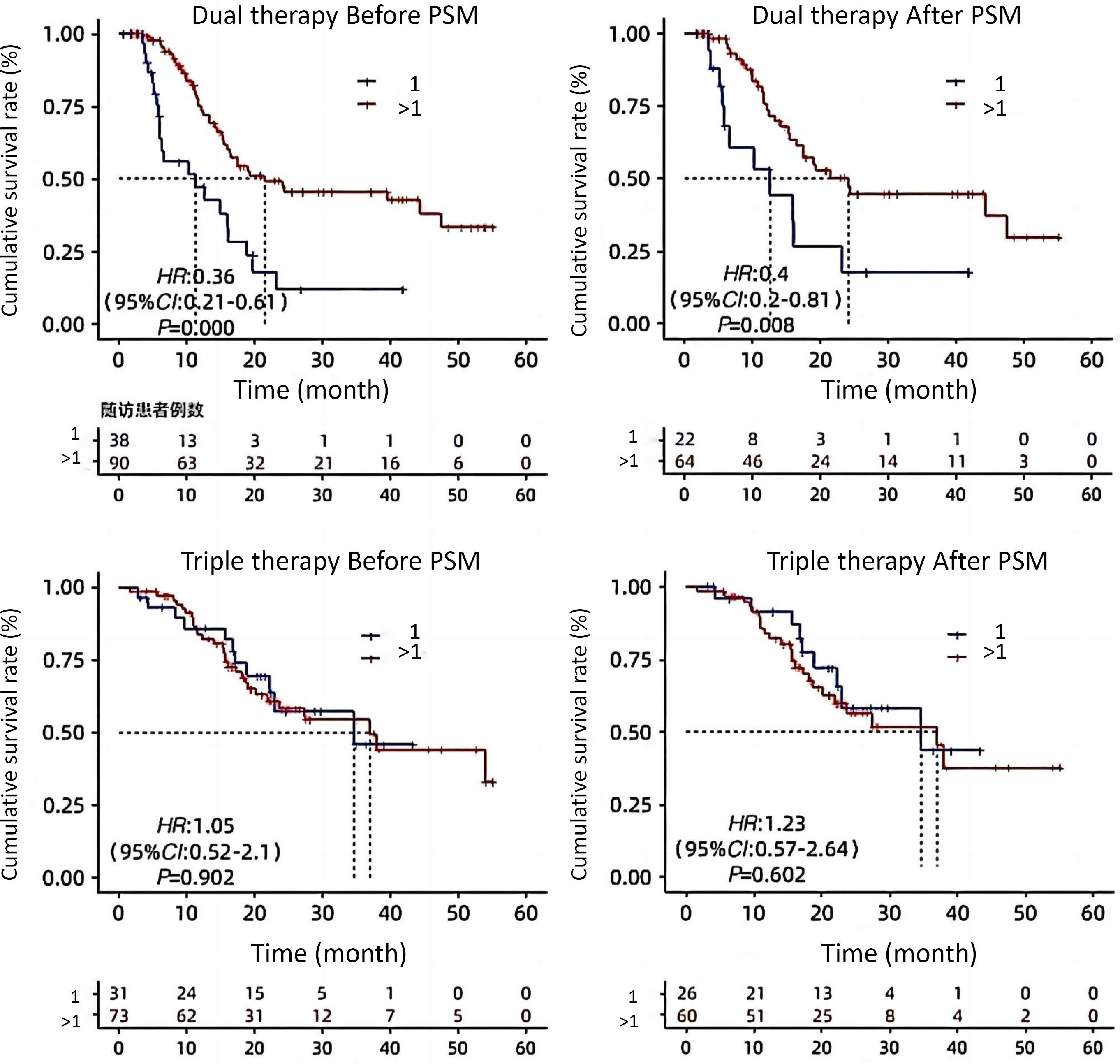
Figure 3.
OS Comparison of the Number of Patients with 1 or More Cases of Cryoablation before and after PSM
.
OS Comparison of the Number of Patients with 1 or More Cases of Cryoablation before and after PSM
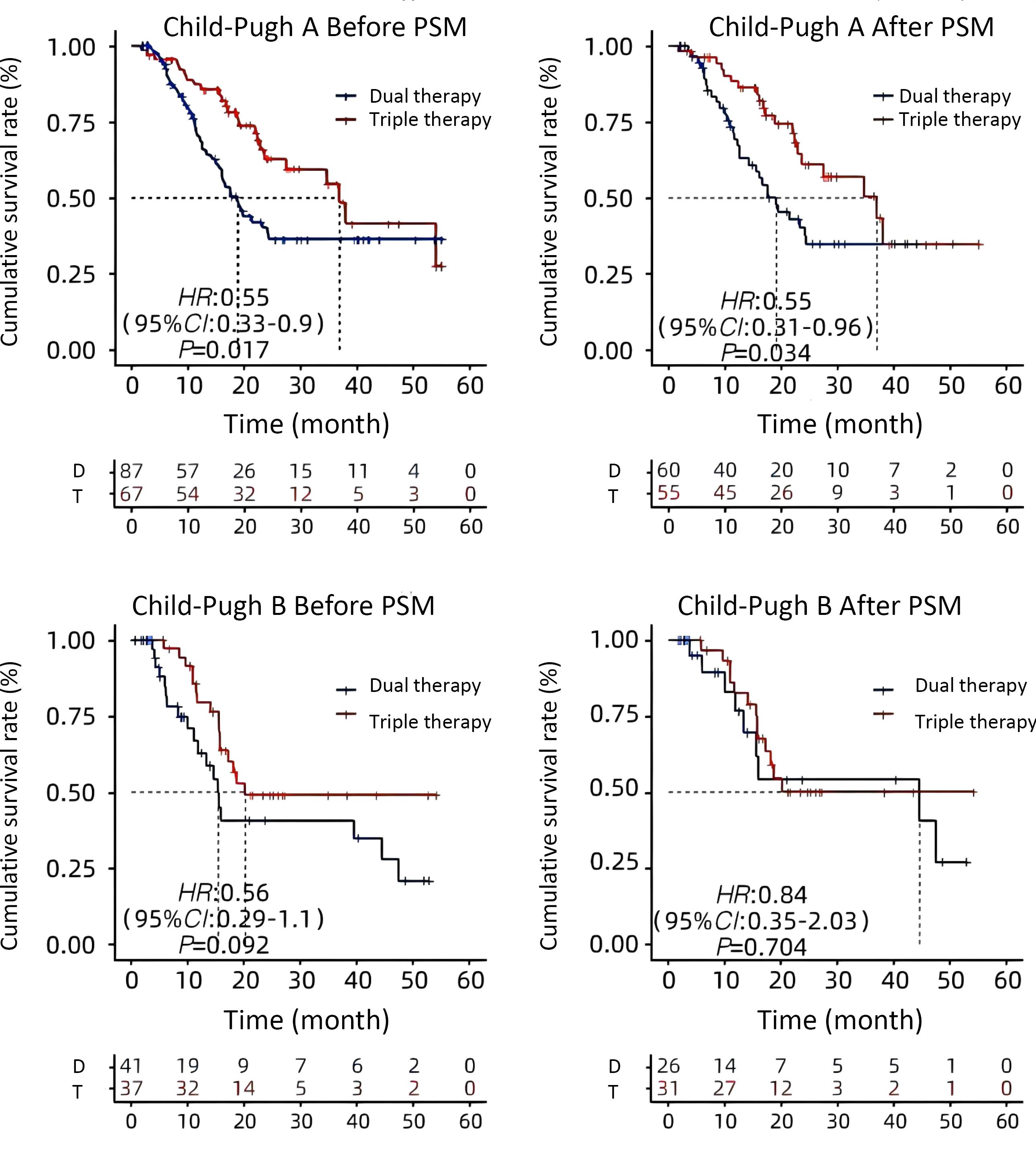
Figure 4.
OS Comparison in Individuals with Child-Pugh Class A or B Disease before and after PSM
.
OS Comparison in Individuals with Child-Pugh Class A or B Disease before and after PSM
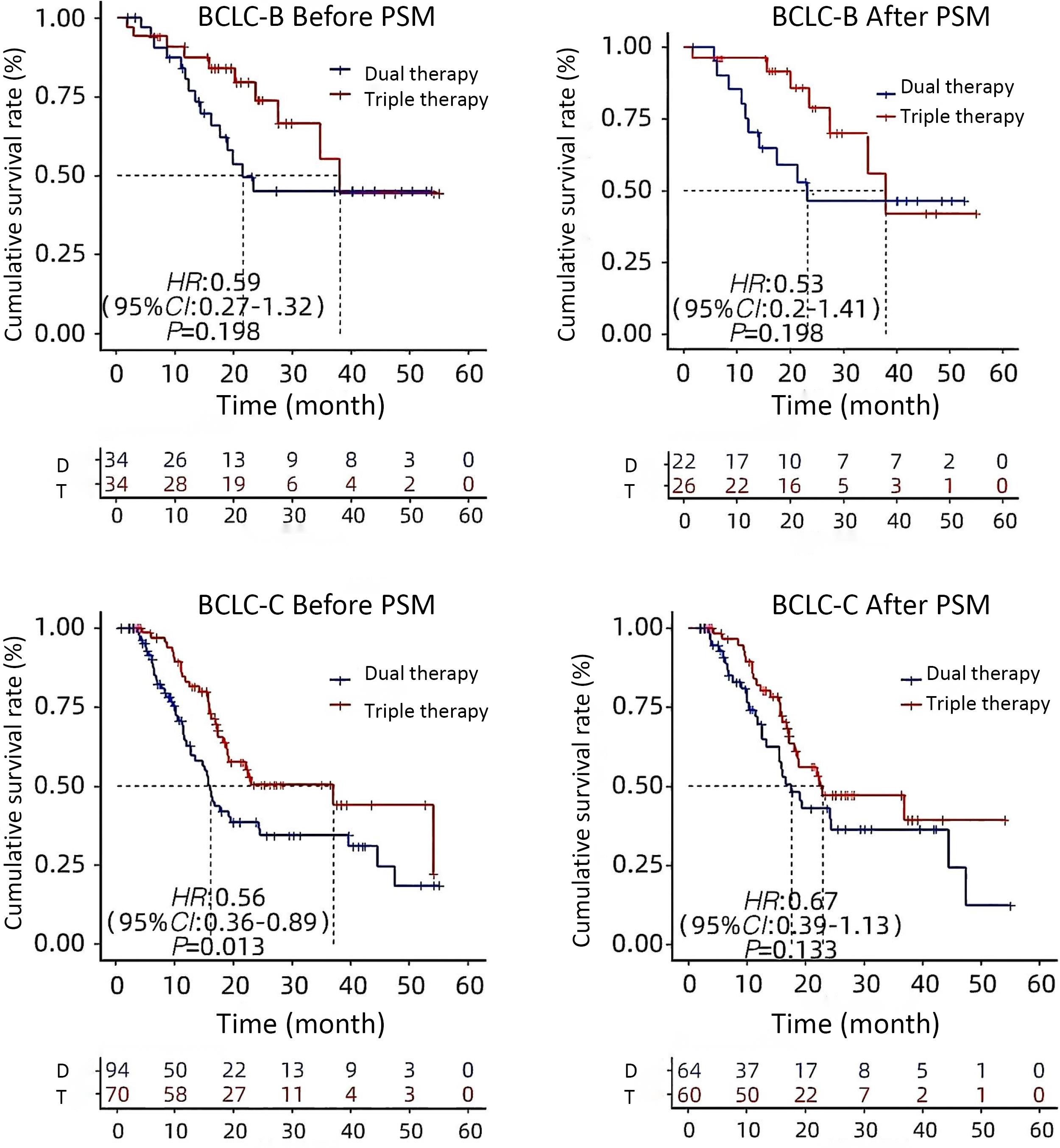
Figure 5.
OS Comparison in BCLC-B or BCLC-C Patients before and after PSM
.
OS Comparison in BCLC-B or BCLC-C Patients before and after PSM
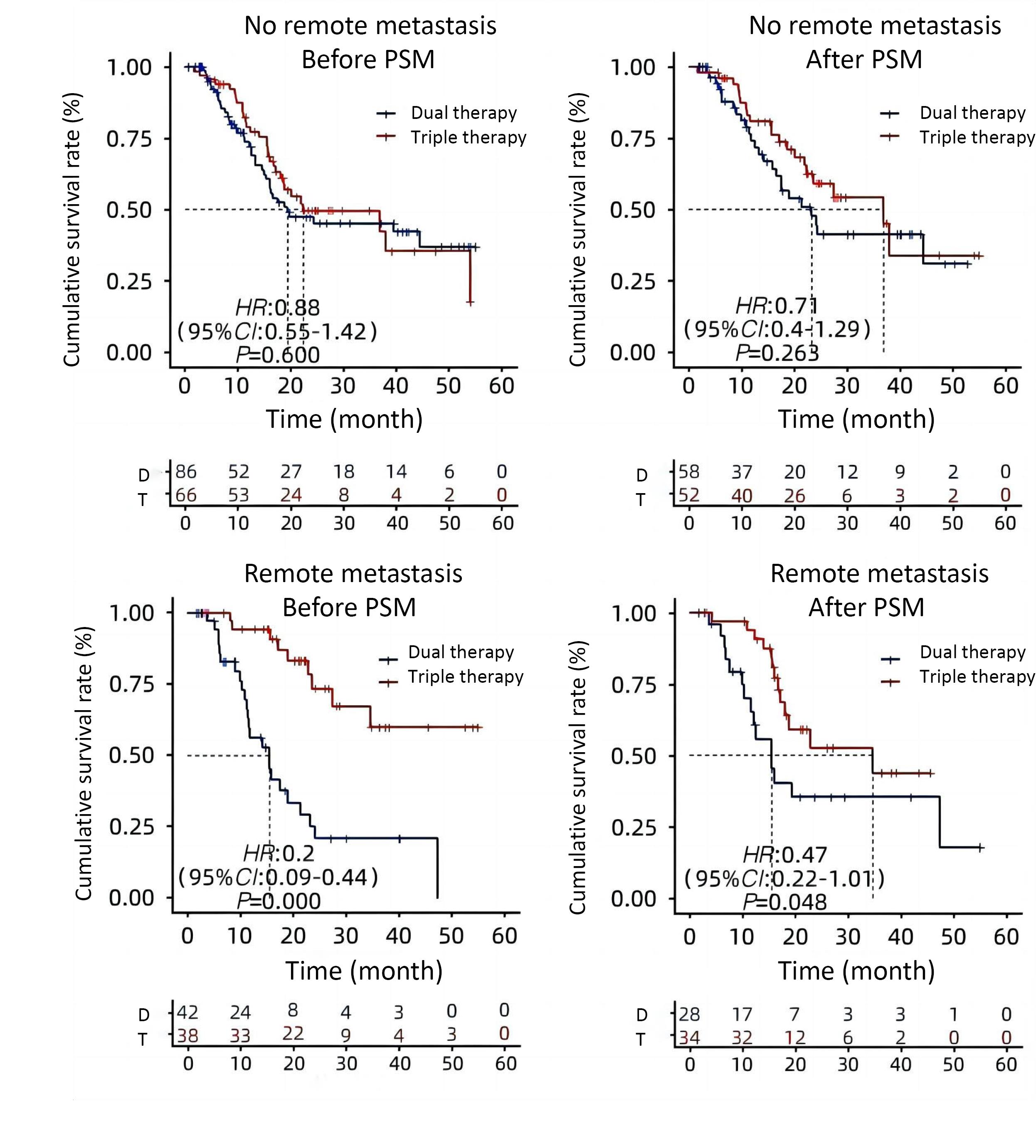
Figure 6.
OS Comparison with or without Distant Metastases Prior to and Following PSM
.
OS Comparison with or without Distant Metastases Prior to and Following PSM
Discussion
Triple therapy consisting of cryoablation plus lenvatinib plus PD-1 mAb may be a better treatment option for patients with advanced HCC. It can also inhibit hypoxia-induced angiogenesis, regulate the tumor immune microenvironment after cryoablation, and enhance the immune response to PD-1 monoclonal antibodies in HCC.18-20 Thus, lenvatinib, PD-1 mAb, and cryoablation together may have a synergistic anticancer effect and improve the clinical prognosis of patients.21
In this study, PD-1 monoclonal antibodies in uHCC patients improved the efficacy of cryoablation combined with renvastinib.22-24 Compared with those in the double group, the median PFS was improved, and the ORR and DCR were also significantly increased.25 Several other studies of local combined system therapy have also shown promising results, and previous studies have evaluated the safety and efficacy of sorafenib combined with cryoablation for advanced HCC.26-28 The results revealed that the median time to disease progression (TTP) was 9.5 months (95% CI: 8.4 ~ 13.5) in the combined treatment group and 5.3 months (95% CI: 3.8 ~ 6.9) in the sorafenib group (P = 0.02). The median OS was 12.5 months (95% CI: 10.6–16.4) in the combined treatment group and 8.6 months (95% CI: 7.3–10.4) in the sorafenib group (P = 0.01). Compared to the control group, patients with high microvascular density (MVD) in the combination therapy group had much longer median TTPs and OS. Other studies evaluated the combined treatment of TACE, renvastinib, and PD-1 inhibitors in uHCC patients, with PFS ranging from 5.2 to 25.2 months and OS ranging from 12.8 to 35.1 months, which was roughly similar to the efficacy of the cryoablation + renvastinib + PD-1 monoclonal antibody protocol in this study. In a study of patients with portal vein cancer thrombus combined with HCC, the ORR in the TACE-HAIC combined with immunotherapy group was significantly greater than that in the TACE group (53.7% vs 7.8%, P < 0.001), and the OS in the combination group was significantly greater than that in the TACE group (P < 0.001). Compared with TACE alone, TACE + cryoablation significantly improved survival in group B (11.0 months vs. 6.0 months, P = 0.08), as did TACE + cryoablation in group C (8.0 months vs. 5.0 months, P = 0.0001). Most of these studies excluded patients with portal vein invasion, distant metastasis or hepatic decompensation, and some included only patients with stage A BCLC. However, the large tumor load in this study (the maximum tumor diameter was 25.3 cm, and most of the tumors had portal vein infiltration or extrahepatic metastasis) may have led to limited survival benefits for these uHCC patients after treatment, and the improvement in PFS was not obvious.29-31 However, in this study, some patients had previously received interventional therapy, local therapy, surgery, other systemic therapy, chemoradiotherapy, or sequential therapy, so the median OS was significantly improved.32-34 Compared to patients receiving double therapy, those with advanced HCC who received triple therapy had a considerably higher survival rate.
According to further subgroup analysis, the median OS of patients with Child‒Pugh grade A HCC with distant metastasis was significantly longer in the triple group than in the double group. OS was prolonged by > 1 case of cryoablation in the double group.35 Therefore, for patients with Child‒Pugh grade A disease and distant metastasis, combining PD-1 monoantibodies with cryoablation and renvastinib is necessary. Adverse events in all triads were manageable and were approximately the same as those reported in previous studies of HCC, with no new or unexpected adverse events observed. In addition, the incidence and severity of adverse events in the triple group were similar to those in the double group without significant differences, suggesting that cryoablation plus renvastinib plus PD-1 mAb did not significantly increase the risk of adverse events, suggesting that the triple regimen had an acceptable safety profile.36
This was a retrospective study conducted in a single medical center and limited in sample size, which may have led to some inherent selection bias, all of which cannot be completely eliminated by PSM analysis.37 Other confounding prognostic factors (such as comorbidities and socioeconomic status) may be present, as well as imperfect matches. Therefore, it is necessary to validate the conclusions of this study through further randomized trials.38-40
In conclusion, this study found that advanced HCC could be safely and effectively treated using cryoablation plus renvastinib plus a PD-1 monoclonal antibody. Patients treated with cryoablation plus renvastinib plus an anti-PD-1 mAb showed a better treatment response and improved survival than patients treated with cryoablation plus renvastinib.
Conclusion
Unresectable liver cancer now has a clinical basis for therapy optimization thanks to cryoablation combination with Renvastinib and PD-1 mAb, which dramatically increased the efficacy and survival of patients with uHCC without increasing adverse effects.
Competing Interests
The authors declare that they have no conflicts of interest.
Ethical Approval
This study has been approved by the Medical Research Ethics Committee (No. HKYS-2025-A0230).
Funding
This work supported by Natural Science Foundation of Fujian Province (2023J011368).
References
- Finn RS, Ikeda M, Zhu AX, Sung MW, Baron AD, Kudo M. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol 2020; 38(26):2960-70. doi: 10.1200/jco.20.00808 [Crossref] [ Google Scholar]
- Yang X, Chen B, Wang Y, Wang Y, Long J, Zhang N. Real-world efficacy and prognostic factors of lenvatinib plus PD-1 inhibitors in 378 unresectable hepatocellular carcinoma patients. Hepatol Int 2023; 17(3):709-19. doi: 10.1007/s12072-022-10480-y [Crossref] [ Google Scholar]
- Wu CJ, Lee PC, Hung YW, Lee CJ, Chi CT, Lee IC. Lenvatinib plus pembrolizumab for systemic therapy-naïve and-experienced unresectable hepatocellular carcinoma. Cancer Immunol Immunother 2022; 71(11):2631-43. doi: 10.1007/s00262-022-03185-6 [Crossref] [ Google Scholar]
- Ishido S, Tsuchiya K, Kano Y, Yasui Y, Takaura K, Uchihara N. Clinical utility of comprehensive genomic profiling in patients with unresectable hepatocellular carcinoma. Cancers (Basel) 2023; 15(3):719. doi: 10.3390/cancers15030719 [Crossref] [ Google Scholar]
- Wang YY, Yang X, Wang YC, Long JY, Sun HS, Li YR. Clinical outcomes of lenvatinib plus transarterial chemoembolization with or without programmed death receptor-1 inhibitors in unresectable hepatocellular carcinoma. World J Gastroenterol 2023; 29(10):1614-26. doi: 10.3748/wjg.v29.i10.1614 [Crossref] [ Google Scholar]
- Wu L, Zheng Y, Liu J, Luo R, Wu D, Xu P. Comprehensive evaluation of the efficacy and safety of LPV/r drugs in the treatment of SARS and MERS to provide potential treatment options for COVID-19. Aging (Albany NY) 2021; 13(8):10833-52. doi: 10.18632/aging.202860 [Crossref] [ Google Scholar]
- Chen S, Xu B, Wu Z, Wang P, Yu W, Liu Z. Pembrolizumab plus lenvatinib with or without hepatic arterial infusion chemotherapy in selected populations of patients with treatment-naive unresectable hepatocellular carcinoma exhibiting PD-L1 staining: a multicenter retrospective study. BMC Cancer 2021; 21(1):1126. doi: 10.1186/s12885-021-08858-6 [Crossref] [ Google Scholar]
- Wu L, Li X, Yan J. Commentary: machine learning developed an intratumor heterogeneity signature for predicting prognosis and immunotherapy benefits in cholangiocarcinoma. Transl Oncol 2024; 45:101995. doi: 10.1016/j.tranon.2024.101995 [Crossref] [ Google Scholar]
- Fu L, Chen P, Wang S, Liu W, Chen Z, Chen H. Complete pathological response with diabetic ketoacidosis to the combination of sintilimab and anlotinib in an unresectable hepatocellular carcinoma patient: a case report. Anticancer Drugs 2022; 33(1):e741-6. doi: 10.1097/cad.0000000000001163 [Crossref] [ Google Scholar]
- Wu L, Zhong Y, Wu D, Xu P, Ruan X, Yan J. Immunomodulatory factor TIM3 of cytolytic active genes affected the survival and prognosis of lung adenocarcinoma patients by multi-omics analysis. Biomedicines 2022; 10(9):2248. doi: 10.3390/biomedicines10092248 [Crossref] [ Google Scholar]
- Wu M, Wang Y, Yang Q, Wang X, Yang X, Xing H. Comparison of baseline 68Ga-FAPI and 18F-FDG PET/CT for prediction of response and clinical outcome in patients with unresectable hepatocellular carcinoma treated with PD-1 inhibitor and lenvatinib. J Nucl Med 2023; 64(10):1532-9. doi: 10.2967/jnumed.123.265712 [Crossref] [ Google Scholar]
- Li ZC, Wang J, Liu HB, Zheng YM, Huang JH, Cai JB. Proteomic and metabolomic features in patients with HCC responding to lenvatinib and anti-PD1 therapy. Cell Rep 2024; 43(3):113877. doi: 10.1016/j.celrep.2024.113877 [Crossref] [ Google Scholar]
- Huang J, Wang ZG, Tao QF, Yang Y, Yuan SX, Gu FM. Efficacy and safety of lenvatinib-based combination therapies for patients with unresectable hepatocellular carcinoma: a single center retrospective study. Front Immunol 2023; 14:1198562. doi: 10.3389/fimmu.2023.1198562 [Crossref] [ Google Scholar]
- Yamashita T, Kudo M, Ikeda K, Izumi N, Tateishi R, Ikeda M. REFLECT-a phase 3 trial comparing efficacy and safety of lenvatinib to sorafenib for the treatment of unresectable hepatocellular carcinoma: an analysis of Japanese subset. J Gastroenterol 2020; 55(1):113-22. doi: 10.1007/s00535-019-01642-1 [Crossref] [ Google Scholar]
- Liu J, Yang L, Wei S, Li J, Yi P. Efficacy and safety of atezolizumab plus bevacizumab versus lenvatinib for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. J Cancer Res Clin Oncol 2023; 149(17):16191-201. doi: 10.1007/s00432-023-05342-5 [Crossref] [ Google Scholar]
- Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat 2011; 10(2):150-61. doi: 10.1002/pst.433 [Crossref] [ Google Scholar]
- Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 2011; 46(3):399-424. doi: 10.1080/00273171.2011.568786 [Crossref] [ Google Scholar]
- Wu L, Liu Q, Ruan X, Luan X, Zhong Y, Liu J. Multiple omics analysis of the role of RBM10 gene instability in immune regulation and drug sensitivity in patients with lung adenocarcinoma (LUAD). Biomedicines 2023; 11(7):1861. doi: 10.3390/biomedicines11071861 [Crossref] [ Google Scholar]
- Fu Z, Li X, Zhong J, Chen X, Cao K, Ding N. Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (uHCC): a retrospective controlled study. Hepatol Int 2021; 15(3):663-75. doi: 10.1007/s12072-021-10184-9 [Crossref] [ Google Scholar]
- Zhu Y, Sun P, Wang K, Xiao S, Cheng Y, Li X. Efficacy and safety of lenvatinib monotreatment and lenvatinib-based combination therapy for patients with unresectable hepatocellular carcinoma: a retrospective, real-world study in China. Cancer Cell Int 2021; 21(1):503. doi: 10.1186/s12935-021-02200-7 [Crossref] [ Google Scholar]
- Wu SJ, Ruan DD, Wu QY, Tang Y, Zhang JH, Cai SL. Safety and efficacy of drug-eluting bead transarterial chemoembolization combined with lenvatinib and anti-PD-1 antibodies for unresectable hepatocellular carcinoma: a retrospective analysis. J Hepatocell Carcinoma 2023; 10:807-20. doi: 10.2147/jhc.S408819 [Crossref] [ Google Scholar]
- Wu L, Zheng Y, Ruan X, Wu D, Xu P, Liu J. Long-chain noncoding ribonucleic acids affect the survival and prognosis of patients with esophageal adenocarcinoma through the autophagy pathway: construction of a prognostic model. Anticancer Drugs 2022; 33(1):e590-603. doi: 10.1097/cad.0000000000001189 [Crossref] [ Google Scholar]
- Yang H, Yang T, Qiu G, Liu J. Efficacy and safety of TACE combined with lenvatinib and PD-(L)1 inhibitor in the treatment of unresectable hepatocellular carcinoma: a retrospective study. J Hepatocell Carcinoma 2023; 10:1435-43. doi: 10.2147/jhc.S423684 [Crossref] [ Google Scholar]
- Chen B, Lei J, Zhao H, Dong J, Zeng Z, Li Y. Efficacy and safety of TKI plus PD-1 inhibitors in elderly uHCC patients: a retrospective study. J Hepatocell Carcinoma 2022; 9:1171-85. doi: 10.2147/jhc.S387254 [Crossref] [ Google Scholar]
- Matsuki M, Hoshi T, Yamamoto Y, Ikemori-Kawada M, Minoshima Y, Funahashi Y. Lenvatinib inhibits angiogenesis and tumor fibroblast growth factor signaling pathways in human hepatocellular carcinoma models. Cancer Med 2018; 7(6):2641-53. doi: 10.1002/cam4.1517 [Crossref] [ Google Scholar]
- Wu L, Zhong Y, Yu X, Wu D, Xu P, Lv L. Selective poly adenylation predicts the efficacy of immunotherapy in patients with lung adenocarcinoma by multiple omics research. Anticancer Drugs 2022; 33(9):943-59. doi: 10.1097/cad.0000000000001319 [Crossref] [ Google Scholar]
- Ogushi K, Chuma M, Uojima H, Hidaka H, Numata K, Kobayashi S. Safety and efficacy of lenvatinib treatment in Child-Pugh A and B patients with unresectable hepatocellular carcinoma in clinical practice: a multicenter analysis. Clin Exp Gastroenterol 2020; 13:385-96. doi: 10.2147/ceg.S256691 [Crossref] [ Google Scholar]
- Furuse J, Izumi N, Motomura K, Inaba Y, Katamura Y, Kondo Y. Safety and effectiveness of lenvatinib in patients with unresectable hepatocellular carcinoma in real-world clinical practice: an observational post-marketing study in Japan. Drugs Real World Outcomes 2023; 10(2):195-205. doi: 10.1007/s40801-022-00348-w [Crossref] [ Google Scholar]
- Li S, Wu J, Wu J, Fu Y, Zeng Z, Li Y. Prediction of early treatment response to the combination therapy of TACE plus lenvatinib and anti-PD-1 antibody immunotherapy for unresectable hepatocellular carcinoma: multicenter retrospective study. Front Immunol 2023; 14:1109771. doi: 10.3389/fimmu.2023.1109771 [Crossref] [ Google Scholar]
- Wu L, Li H, Liu Y, Fan Z, Xu J, Li N. Research progress of 3D-bioprinted functional pancreas and in vitro tumor models. Int J Bioprinting 2024; 10(1):1256. doi: 10.36922/ijb.1256 [Crossref] [ Google Scholar]
- Yamauchi R, Ito T, Yoshio S, Yamamoto T, Mizuno K, Ishigami M. Serum osteopontin predicts the response to atezolizumab plus bevacizumab in patients with hepatocellular carcinoma. J Gastroenterol 2023; 58(6):565-74. doi: 10.1007/s00535-023-01985-w [Crossref] [ Google Scholar]
- Wu L, Li X, Qian X, Wang S, Liu J, Yan J. Lipid nanoparticle (LNP) delivery carrier-assisted targeted controlled release mRNA vaccines in tumor immunity. Vaccines (Basel) 2024; 12(2):186. doi: 10.3390/vaccines12020186 [Crossref] [ Google Scholar]
- Okusaka T, Ikeda K, Kudo M, Finn R, Qin S, Han KH. Safety and efficacy of lenvatinib by starting dose based on body weight in patients with unresectable hepatocellular carcinoma in REFLECT. J Gastroenterol 2021; 56(6):570-80. doi: 10.1007/s00535-021-01785-0 [Crossref] [ Google Scholar]
- Shewarega A, Santana JG, Nam D, Berz A, Tefera J, Kahl V. Effect of incomplete cryoablation and matrix metalloproteinase inhibition on intratumoral CD8 + T-cell infiltration in murine hepatocellular carcinoma. Radiology 2024; 310(2):e232365. doi: 10.1148/radiol.232365 [Crossref] [ Google Scholar]
- Luo J, Dong Z, Xie H, Zhang W, An L, Yu Z. Efficacy and safety of percutaneous cryoablation for elderly patients with small hepatocellular carcinoma: a prospective multicenter study. Liver Int 2022; 42(4):918-29. doi: 10.1111/liv.15169 [Crossref] [ Google Scholar]
- Wu L, Chen X, Zeng Q, Lai Z, Fan Z, Ruan X. NR5A2 gene affects the overall survival of LUAD patients by regulating the activity of CSCs through SNP pathway by OCLR algorithm and immune score. Heliyon 2024; 10(7):e28282. doi: 10.1016/j.heliyon.2024.e28282 [Crossref] [ Google Scholar]
- Gupta P, Maralakunte M, Kumar MP, Chandel K, Chaluvashetty SB, Bhujade H. Overall survival and local recurrence following RFA, MWA, and cryoablation of very early and early HCC: a systematic review and Bayesian network meta-analysis. Eur Radiol 2021; 31(7):5400-8. doi: 10.1007/s00330-020-07610-1 [Crossref] [ Google Scholar]
- Tan J, Liu T, Fan W, Wei J, Zhu B, Liu Y. Anti-PD-L1 antibody enhances curative effect of cryoablation via antibody-dependent cell-mediated cytotoxicity mediating PD-L1(high)CD11b + cells elimination in hepatocellular carcinoma. Acta Pharm Sin B 2023; 13(2):632-47. doi: 10.1016/j.apsb.2022.08.006 [Crossref] [ Google Scholar]
- Wu L, Yang L, Qian X, Hu W, Wang S, Yan J. Mannan-decorated lipid calcium phosphate nanoparticle vaccine increased the antitumor immune response by modulating the tumor microenvironment. J Funct Biomater 2024; 15(8):229. doi: 10.3390/jfb15080229 [Crossref] [ Google Scholar]
- Mandt T, Bangar A, Sauceda C, Das M, Moderbacher C, Ghani M, et al. Stimulating antitumoral immunity by percutaneous cryoablation and combination immunoadjuvant therapy in a murine model of hepatocellular carcinoma. J Vasc Interv Radiol 2023;34(9):1516-27.e6. doi: 10.1016/j.jvir.2023.05.008.