Arch Iran Med. 27(12):707-709.
doi: 10.34172/aim.31604
Case Report
A Rare Anatomical Variation: Intrathoracic Liver Caudate Lobe: A Case Report
Beyza Yaşar Akpınar Conceptualization, Data curation, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing, 1 
Hüseyin Umut Baştürk Conceptualization, Data curation, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing, 1, *
Şeyma Başlılar Conceptualization, Data curation, Investigation, Resources, 1
Yahya Baraç Conceptualization, Data curation, Investigation, Resources, 2
Bengü Şaylan Conceptualization, Data curation, Investigation, Resources, 3
Author information:
1Department of Pulmonary Medicine, University of Health Sciences Sultan Abdulhamid Han Training and Research Hospital, İstanbul, Türkiye
2Department of Radiology, University of Health Sciences Sultan Abdulhamid Han Training and Research Hospital, İstanbul, Türkiye
3Department of Pulmonary Medicine, University of Health Sciences Süreyyapaşa Training and Research Hospital, İstanbul, Türkiye
Abstract
We present a case with an intrathoracic caudate lobe in a 45-year-old woman who referred with a complaint of nonspecific chest pain. She denied previous history of trauma or surgery. Computed tomography (CT) pulmonary angiography showed a paravertebral, soft tissue mass which raised suspicion of a pleural tumor. In the coronal plane, the mass was protruding to the abdomen and had similar density with liver. Magnetic resonance imaging confirmed the diagnosis.
Keywords: Chest pain, Computed tomography, Liver caudate lobe, Magnetic resonance imaging
Copyright and License Information
© 2024 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Akpınar BY, Baştürk HU, Başlılar Ş, Baraç Y, Şaylan B. A rare anatomical variation: intrathoracic liver caudate lobe: a case report. Arch Iran Med. 2024;27(12):707-709. doi: 10.34172/aim.31604
Introduction
The intrathoracic abnormally positioned liver lobe is an extremely rare anomaly which may be misdiagnosed as a mediastinal mass, pulmonary sequestration, esophageal cyst, hydatid cyst and pleural or lung tumor. The first case was described in 19571 and, since then, about 30 case reports have been published.2-4 The most frequent symptoms are cough, respiratory distress and chest pain; but hemoptysis, dyspnea and abdominal pain have been also reported,2 while there are a few asymptomatic cases diagnosed incidentally5,6 or during autopsy.7,8 It may be a developmental anomaly or the liver tissue may protrude into the thoracic cavity following trauma or surgery.
Contrast enhanced thorax computed tomography (CT), CT-angiography, and magnetic resonance imaging (MRI) are useful in making the diagnosis. However, in most cases, the diagnosis is made surgically (thoracotomy/laparotomy). We present a case with an intrathoracic accessory caudate lobe in a 45-year-old woman who referred with a nonspecific chest pain. CT showed a paravertebral, ellipsoid, well-circumscribed homogeneous soft tissue mass which raised suspicion of a pleural tumor. In the coronal plane, the mass was protruding to the abdomen and had similar density with liver. The diagnosis was confirmed with contrast-enhanced MRI of the thorax and abdomen which showed the mass to be connected with a small pedicle to the orthotopic liver.
Case Report
A 45-year-old female patient visited the emergency room with a right sided non-specific chest pain which she experienced when she became excited. She was an active smoker (15 pack-years) and used oral contraceptives and anxiolytics regularly. There was a family history of malignancy. CT-pulmonary angiography was requested due to the suspicion of pulmonary thromboembolism which showed no thrombus in pulmonary arteries but reported a mass lesion at the base of the right hemithorax (Figure 1). A Positron emission tomography–computed tomography (PET-CT) scan was requested which did not show any pathological fluorodeoxyglucose (FDG) uptake (SUV max: 2,1). So she was referred to our clinic. Her physical examination was unremarkable. The patient’s CT images were reevaluated; the mass was paravertebrally placed, ellipsoid, well-circumscribed and homogeneous. In the coronal plane, the mass was protruding to the abdomen and had similar density with liver (Figure 1). The patient was referred to the radiology clinic with a preliminary diagnosis of intrathoracic ectopic liver. In line with the suggestion of the radiologist, a contrast enhanced magnetic resonance imaging of the thorax and upper abdomen was performed. The mass was connected with a small pedicle to the orthotopic liver and had similar and continuous vascularity with the liver, showed similar contrast enhancement with the liver parenchyma on the contrast-enhanced fat-suppressed T1-weighted sequence, and had anatomical continuity with the caudate lobe (Figure 2). So, it was concluded that this mass was an intrathoracic liver caudate lobe.
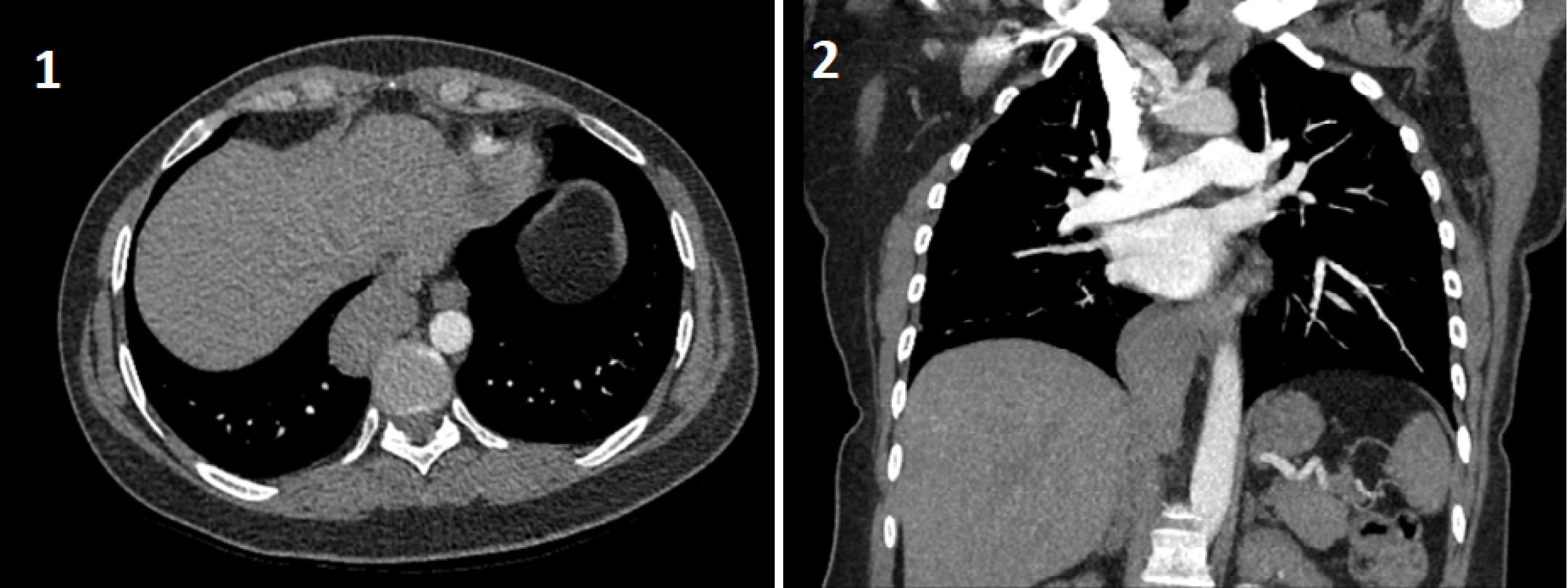
Figure 1.
1) Non-contrast chest-CT imaging in transverse section. 2) Contrast-enhanced CT-pulmonary angiography image in coronal section
.
1) Non-contrast chest-CT imaging in transverse section. 2) Contrast-enhanced CT-pulmonary angiography image in coronal section
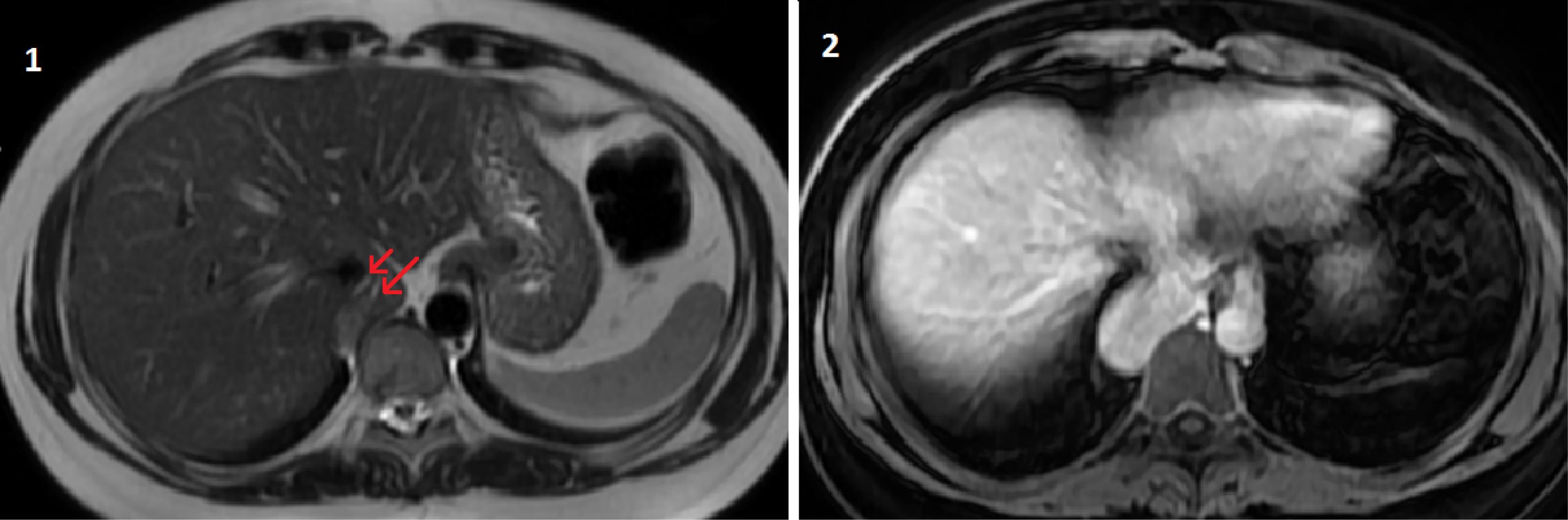
Figure 2.
1) Vascular structures marked with red arrows, similar to liver tissue and extending into the hiatus, on the T2-weighted sequence. 2) Lesion showing similar enhancement as liver parenchyma on contrast-enhanced fat-suppressed T1-weighted sequence
.
1) Vascular structures marked with red arrows, similar to liver tissue and extending into the hiatus, on the T2-weighted sequence. 2) Lesion showing similar enhancement as liver parenchyma on contrast-enhanced fat-suppressed T1-weighted sequence
Discussion
The intrathoracic displacement of a liver lobe was first reported by Hansbrough and Lipin 1 nearly seventy years ago but the classification of this anomaly was defined recently by Adin et al as follows: Type I: herniated liver tissue through a diaphragmatic defect; Type II: supradiaphragmatic liver mass connected to the liver through a vasculobiliary pedicle; and Type III: ectopic liver tissue separated from the liver, generally more distant. Type II has been reported as the most common, and type III the least common.9 Types I and II were termed as accessory liver lobe while the last type was termed as ectopic liver as it has no connection to the orthotopic liver. Our case was consistent with type II anomaly.
The accessory liver may protrude into the thoracic cavity via diaphragmatic defects or through the inferior vena cava foramen.2,5 Most of the reported cases were placed in the right hemithorax. Although it was suggested that the liver tissue may be displaced following surgery or trauma, the majority of cases were suggested to be developmental.2 It was brought forward that in case of developmental anomalies, an accessory liver lobule was developed and the original one became atrophied.4 Some of the cases were reported to accompany other anomalies such as pulmonary sequestrations, arterio-venous malformations and cardiac anomalies.2-5,8,10
According to the literature, most of the cases referred with complaints of chest/abdominal pain and respiratory distress. Furthermore, symptoms related to the accompanying anomalies such as productive cough and recurrent pneumonia in case of accompanying pulmonary sequestrations were also reported2. On the other hand, some of the cases were detected incidentally or during autopsy.3-5,7,8 Most of the cases reported in the literature were misdiagnosed as tumors, pulmonary sequestration or cysts; thus, the diagnosis was made via unnecessary thoracotomies or laparotomies.2 Adin et al proposed that the diagnosis may be made easily with all imaging techniques in case of type I and II anomalies and ultrasound examination should be preferred in the pediatric population to avoid irradiation.9 For radiological diagnosis, multiplanar reconstruction of the CT scans is important which may show the vascularity and the connection of the ectopic tissue to the orthotopic liver. In our case, the CT scan showed a well-circumscribed, homogeneous mass in the base of right hemithorax which had a similar density with the normal liver tissue. In coronal plane sections, the mass was connected to the caudal lobe of the liver. The MRI sequences supported our diagnosis visualizing the vascularization and connection of the mass to the liver more precisely.
An intrathoracic ectopic or accessory liver lobe is usually clinically insignificant, so no intervention is necessary unless there is a concomitant anomaly which requires surgical treatment such as pulmonary sequestration. However, most of the cases in the literature underwent unnecessary surgeries such as thoracotomy or laparotomy.
We presented this case to emphasize that the intrathoracic ectopic liver should be kept in mind in differential diagnosis of mass lesions adjacent to the diaphragm. The diagnosis may be achieved by noninvasive imaging techniques which may prevent unnecessary interventions and surgical complications.
Competing Interests
The authors have no conflict of interest to declare.
Data Availability Statement
The data that support the inferences of this case presentation are available upon reasonable request from the corresponding author.
Ethical Approval
Each procedure executed in this study was compatible with the ethical norms of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or analogous ethical norms. Informed consent was procured from the patient at every treatment step throughout the entire treatment process in which a healthcare professional educated the patient about the risks, benefits, and alternatives of a given procedure or intervention. The authors assure that all appropriate patient consent forms in which the patient has bestowed her/his consent for clinical information to be announced in the journal were obtained. The patients comprehend that her/his name and initials will never be disclosed and due endeavors will be performed to censor her/his identity, but no anonymity can be pledged.
Funding
The authors declare that they have definitely no competing financial interests or personal relationships that could have influenced this paper.
References
- Hansbrough ET, Lipin RJ. Intrathoracic accessory lobe of the liver. Ann Surg 1957; 145(4):564-7. doi: 10.1097/00000658-195704000-00014 [Crossref] [ Google Scholar]
- Chen YY, Huang TW, Chang H, Hsu HH, Lee SC. Intrathoracic caudate lobe of the liver: a case report and literature review. World J Gastroenterol 2014; 20(17):5147-52. doi: 10.3748/wjg.v20.i17.5147 [Crossref] [ Google Scholar]
- Jhamb S, Pillai H, Maguire C, Palamuthusingam P. Incidental finding of heterotopic supradiaphragmatic liver. J Surg Case Rep 2020; 2020(10):rjaa394. doi: 10.1093/jscr/rjaa394 [Crossref] [ Google Scholar]
- Sakarya A, Erhan Y, Aydede H, Kara E, Ilkgül O, Ciftdoğan C. Ectopic liver (choristoma) associated with the gallbladder encountered during laparoscopic cholecystectomy: a case report. Surg Endosc 2002; 16(7):1106. doi: 10.1007/s00464-001-4251-5 [Crossref] [ Google Scholar]
- ‘Errico F, Laudazi M, Pitaro M, Pietropaolo A, Paoloantonio P, Garaci F. Incidental finding of intrathoracic caudate lobe of the liver associated with an arterovenous malformation. Radiol Case Rep 2023; 18(3):1186-9. doi: 10.1016/j.radcr.2022.12.008 [Crossref] [ Google Scholar]
- Ihara K, Isono H. Accessory liver lobe in the right thoracic cavity. J Gen Fam Med 2022; 23(5):351-3. doi: 10.1002/jgf2.546 [Crossref] [ Google Scholar]
- Shah KD, Beck AR, Jhaveri MK, Keohane M, Weinberg B, Gerber MA. Infantile hemangioendothelioma of heterotopic intrathoracic liver associated with diaphragmatic hernia. Hum Pathol 1987; 18(7):754-6. doi: 10.1016/s0046-8177(87)80250-2 [Crossref] [ Google Scholar]
- Shapiro JL, Metlay LA. Heterotopic supradiaphragmatic liver formation in association with congenital cardiac anomalies. Arch Pathol Lab Med 1991; 115(3):238-40. [ Google Scholar]
- Adin ME, Çetinçakmak MG, Deniz MA, Göya C. Accessory liver within the thoracic cavity. Surg Radiol Anat 2018; 40(9):1085-91. doi: 10.1007/s00276-018-2046-9 [Crossref] [ Google Scholar]
- Choi SU, Kim HK, Kim J. Heterotopic supradiaphragmatic liver combined with intralobar pulmonary sequestration. Ann Thorac Surg 2008; 85(5):1809-10. doi: 10.1016/j.athoracsur.2007.11.040 [Crossref] [ Google Scholar]