Arch Iran Med. 24(12):897-902.
doi: 10.34172/aim.2021.134
Original Article
Hazard Ratio of 90-Day Mortality in ICU Patients with Abdominal Injuries Compared with Head Injuries
Farshid Rahimi-Bashar 1  , Sara Ashtari 2 , Ali Fathi Jouzdani 3, Seyed Jalal Madani 4, * , Keivan Gohari-Moghadam 5, *
, Sara Ashtari 2 , Ali Fathi Jouzdani 3, Seyed Jalal Madani 4, * , Keivan Gohari-Moghadam 5, *
Author information:
1Department of Anesthesiology and Critical Care, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
2Gastroenterology and Liver Diseases Research Center, Research Institute for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Student Research Committee, Hamadan University of Medical Sciences, Hamadan, Iran
4Trauma Research Center, Medicine Faculty, Baqiyatallah University of Medical Sciences, Tehran, Iran
5Medical ICU and Pulmonary Unit, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran
*Corresponding Authors: Seyed Jalal Madani, MD; Trauma Research Center, Medicine Faculty, Baqiyatallah University of Medical Sciences, P.O. Box 19575-174,
Sheykh Bahayi Stress, Vanak Square, Tehran, Iran. Tel:+98-919-6017138; Fax:+98-21-8755487;
Email:
dr.jalalmadani@gmail.com. Keivan Gohari-Moghadam,
MD; Medical ICU and Pulmonary unit, Shariati hospital, Tehran University of Medical Sciences, P.O. Box 14117-13135, Jalal-e-Al-e-Ahmad Hwy, Tehran, Iran.
Email:
kgohari@tms.ac.ir
Abstract
Background:
Despite advances in the treatment of abdominal injuries in patients with trauma, it remains a major public health problem worldwide. Evaluation of hazard ratio (HR) of 90-day mortality in intensive care unit (ICU) patients with abdominal injuries compare with head injuries in trauma patients and non-trauma surgical ICU patients.
Methods:
This single-center, prospective cohort study was conducted on 400 patients admitted to the ICU between 2018 and 2019 due to trauma or surgery in Hamadan, Iran. The main outcome was mortality at 90-day after ICU admission. Cox proportional hazards models were used to determine the HR and 95% confidence interval (CI) for 90-day mortality.
Results:
The 90-day mortality was 21.9% in abdominal injuries patients. According to multivariate Cox regression, the expected hazard mortality was 2.758 times higher in patients with abdominal injuries compared to non-trauma patients (HR: 2.758, 95% CI: 1.077–7.063, P = 0.034). About more than 50% of all deaths in the abdominal and head trauma groups occurred within 20 days after admission. Mean time to death was 27.85±20.1, 30.27±18.22 and 31.43±26.24 days for abdominal-trauma, surgical-ICU, and head-trauma groups, respectively.
Conclusion:
Difficulty in accurate diagnosis due to the complex physiological variability of abdominal trauma, less obvious clinical symptoms in blunt abdominal injuries, multi-organ dysfunction in abdominal injuries, failure to provide timely acute care, as well as different treatment methods all account for the high 90-day mortality rate in abdominal-trauma patients. Therefore, these patients need a multidisciplinary team to care for them both in the ICU and afterwards in the general ward.
Keywords: Abdominal trauma, Failure to rescue, Head trauma, Mortality
Copyright and License Information
© 2021 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Rahimi-Bashar F, Ashtari S, Fathi Jouzdani A, Madani SJ, Gohari-Moghadam K. Hazard ratio of 90-day mortality in icu patients with abdominal injuries compared with head injuries. Arch Iran Med. 2021;24(12):897-902. doi: 10.34172/aim.2021.134
Introduction
Abdominal injury is a common cause of death in the first 40 years of life. Regardless of the level of socio-economic development, it remains a major public health problem in all countries.1 Abdomen, which includes the stomach, small intestine, large intestine, liver, pancreas, gallbladder and kidneys, is the third most frequently injured body region and about 25% of all abdominal trauma cases require surgery. Generally, abdominal injuries are caused by blunt or penetrating injuries, and approximately 7–10% of trauma-related deaths are caused by these injuries.2,3 Vehicle or road accidents, falling from a height, and interpersonal violence are common causes of blunt abdominal trauma.4-6 However, the most common causes of penetrating abdominal trauma are stabbing and gunshot.7-9
Most hospitalized patients with abdominal injuries die during initial care in an emergency room or ICU. However, many patients lose their lives after being discharged from the intensive care unit (ICU). On first sight, these cases can be treated as “failure to rescue” of potential recoverable patients.10 Despite advances in the treatment of abdominal injuries in trauma patients, in the field of prehospital care, emergency department (ED) care, surgical techniques and intensive care, the high mortality rate in these patients remains a challenge for public health.11,12 Through the use of warning scores and other system monitoring tools or implementation of emergency medical teams, early detection of patients at risk can be achieved.13,14 Due to the physiological diversity of abdominal injuries in trauma patients, it may be difficult or even impossible to distinguish between preventable complications and side effects from the “normal course of trauma”. Thus, reliable rates of failure to rescue are still lacking.15,16 In order to observe and measure the quality of care in the ICU, one approach could be to analyze severely injured patients who die after an initial treatment in an ICU.
To date, no studies have been performed to evaluate the 90-day mortality of abdominal injuries in ICU trauma patients compared to other non-trauma ICU patients (surgical population) or even patients with other types of injuries (head injuries). Therefore, we conducted this study to determine the survival of patients with abdominal injuries and compare it with the analysis of patients with head injuries as well as a surgical critically ill population in the ICU. The main outcome was mortality at 90 days after ICU admission.
Materials and Methods
Study Design
From January 2018 to December 2019, we enrolled a total of 400 patients with abdominal injuries and head injuries as trauma patients, as well as non-trauma surgical patients who were admitted to the mixed medical-surgical ICU at the Be’sat Hospital in Hamadan, Iran. This prospective observational study was conducted and reported in accordance with the recommendations of the STROBE statement.17
Eligibility Criteria
Eligibility was limited to those patients who were over 18 years of age who were hospitalized for longer than 24 hours in the ICU due to abdominal injuries, head injuries or surgery.
Outcome Measurement
The main outcome was 90-day mortality, measured from the patient’s ICU admission date.
Data Collection
A well-trained intensive care physician was assigned for data collection (F.R-B). The demographic data collected included age, sex, marital status, and smoking status, based on the medical records of all eligible ICU patients. The severity of illness was measured by the Acute Physiology and Chronic Health Evaluation (APACHE)-IV.18,19 The APACHE IV score was calculated in the first 24 hours of admission to the ICU. The worst values of vitals and laboratory parameters were considered for calculating the score. The score was calculated using the online calculator (http://intensivecarenetwork.com/Calculators/Files/Apache4.html). ICU length of stay (LOS) was recorded for each patient. In addition, after ICU discharge, the status of all patients was followed for 90 days (three months) via phone contacts by researchers every 10 days.
Statistical Analysis
Categorical variables were described as frequency rates and percentages. Continuous variables were described using mean ± standard deviation (SD) values. ANOVA was used to compare the demographic and clinical data across the three study groups. Moreover, the mean scores of age, APACHE IV, and ICU LOS were compared between the two groups using Bonferroni’s post hoc test. Univariate and multivariate Cox’s proportional hazards models, with 90-day mortality as the event and the time to onset of death, were used to assess survival. Finding were reported as hazard ratio (HR) with 95% confidence intervals (CI) and P values. In addition, the Kaplan-Meier curve was used to visually represent and compare survival and hazard functions for all three groups of study. All data were analyzed using the Statistical Package for the Social Sciences (SPSS) 21.0 statistical package (Chicago, IL, USA), and two-sided P < 0:05 indicated a statistically significant difference.
Results
Demographic, Clinical and Outcome Characteristics of Patients
From January 2018 to December 2019, a total of 400 critically ill patients due to trauma or non-trauma in the mixed medical-surgical ICU at the Be’sat Hospital in Hamadan, Iran, met the inclusion criteria. Of 400 participants, 176 (44%) patients were admitted to the ICU due to head trauma, 126 (32%) patients due to abdominal trauma and 96 (24%) patients due to surgery. Baseline characteristics and outcomes of the participants according to three study groups are presented in Table 1. There was a statistically significant difference between the three groups in terms of age (P < 0.001), sex (P < 0.001), mean score of APACHE IV (P < 0.001), length of ICU stay (P < 0.001), as well as 90-day mortality rate (P = 0.041). According to the results, significantly more males than females were present in the abdominal trauma (82.8% vs 17.2%, P < 0.05) group.
Table 1.
Baseline Characteristics and Outcomes of the Participants According to the Three Study Groups
| Variables |
Head Trauma
Patients (n=176)
|
Abdominal Trauma Patients (n=128)
|
Non-trauma Patients (n=96)
|
P
Value
|
| Age |
Mean ± SD (years) |
31.83 ± 9.86 |
33.92 ± 7.70 |
50.35 ± 10.22 |
< 0.001* |
| Range (min-max) |
(18–56) |
(24–45) |
(28–66) |
| Gender |
Male (%) |
98 (55.7) |
106 (82.8) |
54 (56.2) |
< 0.001* |
| Female (%) |
78 (44.3) |
22 (17.2) |
42 (43.7) |
Marital
Status |
Married (%) |
108 (61.4) |
79 (61.7) |
57 (59.4) |
0.930 |
| Unmarried (%) |
46 (26.1) |
34 (26.6) |
26 (27.1) |
| Divorce (%) |
22 (12.5) |
15 (11.7) |
13 (13.5) |
| Smoking |
1 Pocket per week (%) |
39 (22.2) |
26 (20.3) |
21 (21.9) |
0.610 |
| > 1 Pocket per week (%) |
72 (40.9) |
49 (38.3) |
41 (42.7) |
| No smoking (%) |
65 (36.9) |
53 (41.4) |
34 (35.4) |
| APACHE IV, Score, Mean ± SD |
6.63 ± 1.211 |
13.39 ± 3.411 |
10.10 ± 3.649 |
< 0.001* |
| ICU LOS, Mean ± SD (days) |
5.011 ± 1.296 |
12.343 ± 4.147 |
7.583 ± 2.728 |
< 0.001* |
| Outcome |
Alive (%) |
153 (89.6) |
100 (78.1) |
85 (88.5) |
0.041* |
| Death (%) |
23 (13.1) |
28 (21.9) |
11 (11.5) |
APACHE, Acute Physiology and Chronic Health Evaluation; LOS, length of stay; ICU, intensive care unit.
*P < 0.05 considered as significant.
In terms of age, no significant difference was observed between patients with head injuries and abdominal injuries (31.83 ± 9.86 vs. 33.92 ± 7.70, P = 0.161) in the trauma patients groups. However, the mean age of non-trauma patients was significantly higher than that of patients with head and abdominal trauma (P < 0.001). Mean score of APACHE IV and the mean ICU LOS in patients with abdominal-trauma was significantly higher than that of patients with head trauma and non-trauma patients (P < 0.001). However, the mean score of APACHE IV (6.63 ± 1.211 vs. 10.10 ± 3.649, P < 0.001) and the mean ICU LOS (5.011 ± 1.296 vs. 7.583 ± 2.728, P < 0.001) in patients with head trauma was significantly lower than that of non-trauma patients. According to the results, the 90-day mortality rate in patients with abdominal trauma was significantly higher than the mortality rate in patients with head trauma and non-trauma patients (P = 0.041).
Proportional Hazard Cox Regression Findings
A proportional hazard Cox regression analysis with time-varying covariates, taking 90-day mortality as the event, and the time to onset of mortality was used in the study, as listed in Table 2. Univariate Cox regression analysis showed that the abdominal injuries in trauma patients (HR: 1.991, 95% CI: 0.991–3.999, P = 0.043), high score of APACHE IV (HR: 1.08, 95% CI: 1.019–1.144, P = 0.009), and longer stay in the ICU (HR: 1.05, 95% CI: 1.002–1.112, P = 0.043), were significantly associated with mortality. According to multivariate Cox regression, the expected hazard mortality was 2.758 times higher in patients with abdominal injuries compared to non-trauma patients (HR: 2.758, 95% CI: 1.077–7.063, P = 0.034). The Kaplan-Meier curves of survival for three groups of study are shown in Figure 1. As can be seen, the survival of patients with abdominal trauma was lower than the other two groups of patients, while the survival of patients with head trauma and non-trauma patients was almost the same. In addition, survival time was compared across the groups using the log-rank test (Figure 2).
Table 2.
Proportional Hazard Cox Regression Analysis of 90-day Mortality in Trauma and Non-trauma Patients
|
Variables
|
Univariate
|
Multivariate
|
|
HR (95% CI)
|
P
Value
|
HR (95% CI)
|
P
Value
|
| Group (head trauma vs. non-trauma) |
1.141 (0.556–2.340) |
0.719 |
2.401 (0.926–6.223) |
0.072 |
| Group (abdominal trauma vs. non-trauma) |
1.991 (0.991–3.999) |
0.043* |
2.758 (1.077–7.063) |
0.034* |
| Age |
1.011 (0.99–-1.031) |
0.300 |
1.026 (0.998–1.054) |
0.069 |
| Gender (female vs. male) |
1.272 (0.728–2.222) |
0.398 |
0.919 (0.500–1.688) |
0.787 |
| Marital status (unmarried vs. married) |
1.488 (0.867–2.553) |
0.149 |
1.451 (0.837–2.518) |
0.185 |
| Smoking (yes vs. no) |
0.813 (0.491–1.347) |
0.422 |
1.260 (0.752–2.112) |
0.380 |
| APACHE IV score |
1.080 (1.019–1.144) |
0.009* |
1.117 (0.982–1.270) |
0.092 |
| ICU LOS |
1.056 (1.002–1.112) |
0.043* |
0.949 (0.844–1.067) |
0.380 |
APACHE, Acute Physiology and Chronic Health Evaluation; LOS, length of stay; ICU, intensive care unit.
*
P < 0.05 considered as significant.
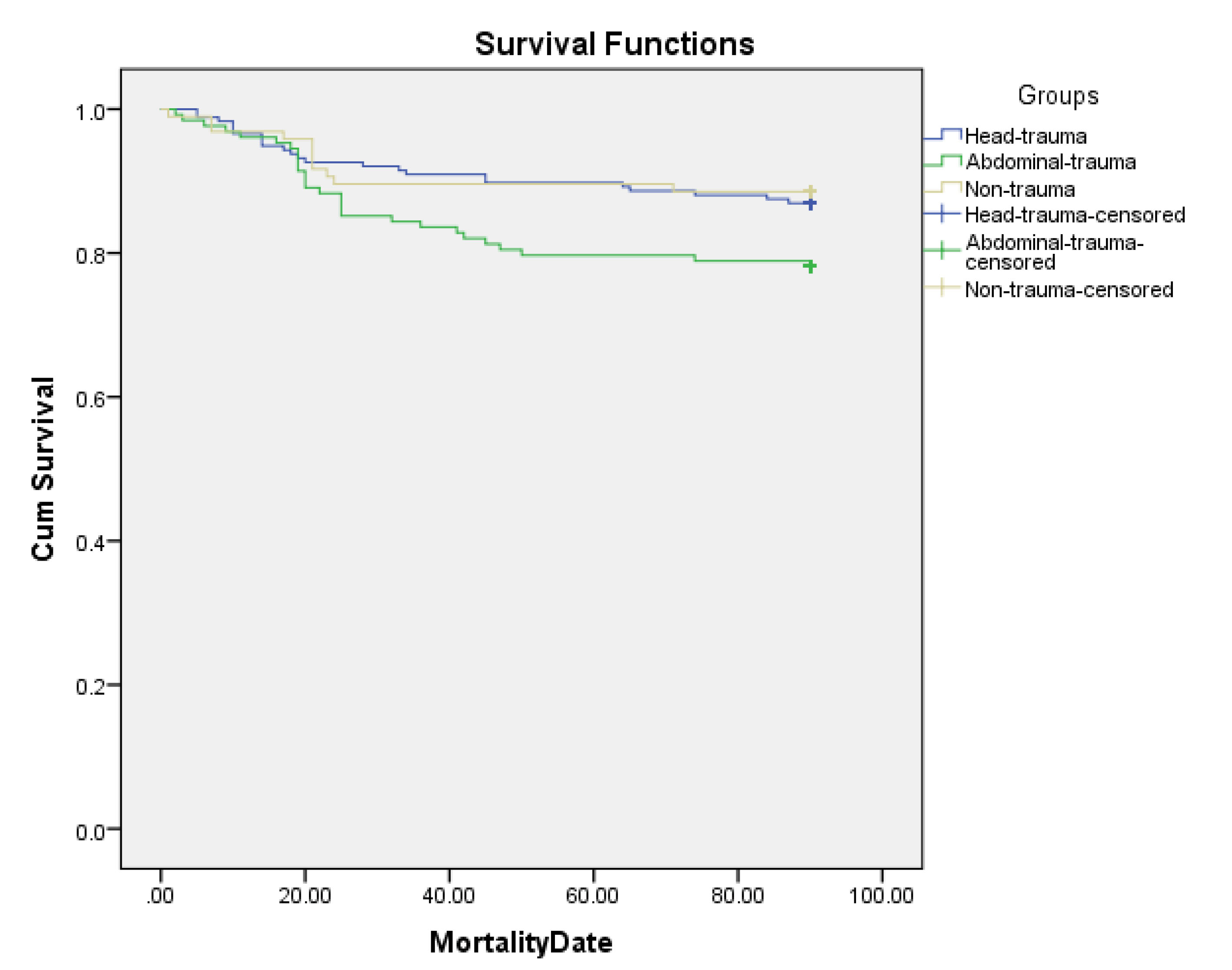
Figure 1.
Kaplan-Meier Survival Analysis of 90-Day Mortality in the Three Study Groups.
.
Kaplan-Meier Survival Analysis of 90-Day Mortality in the Three Study Groups.
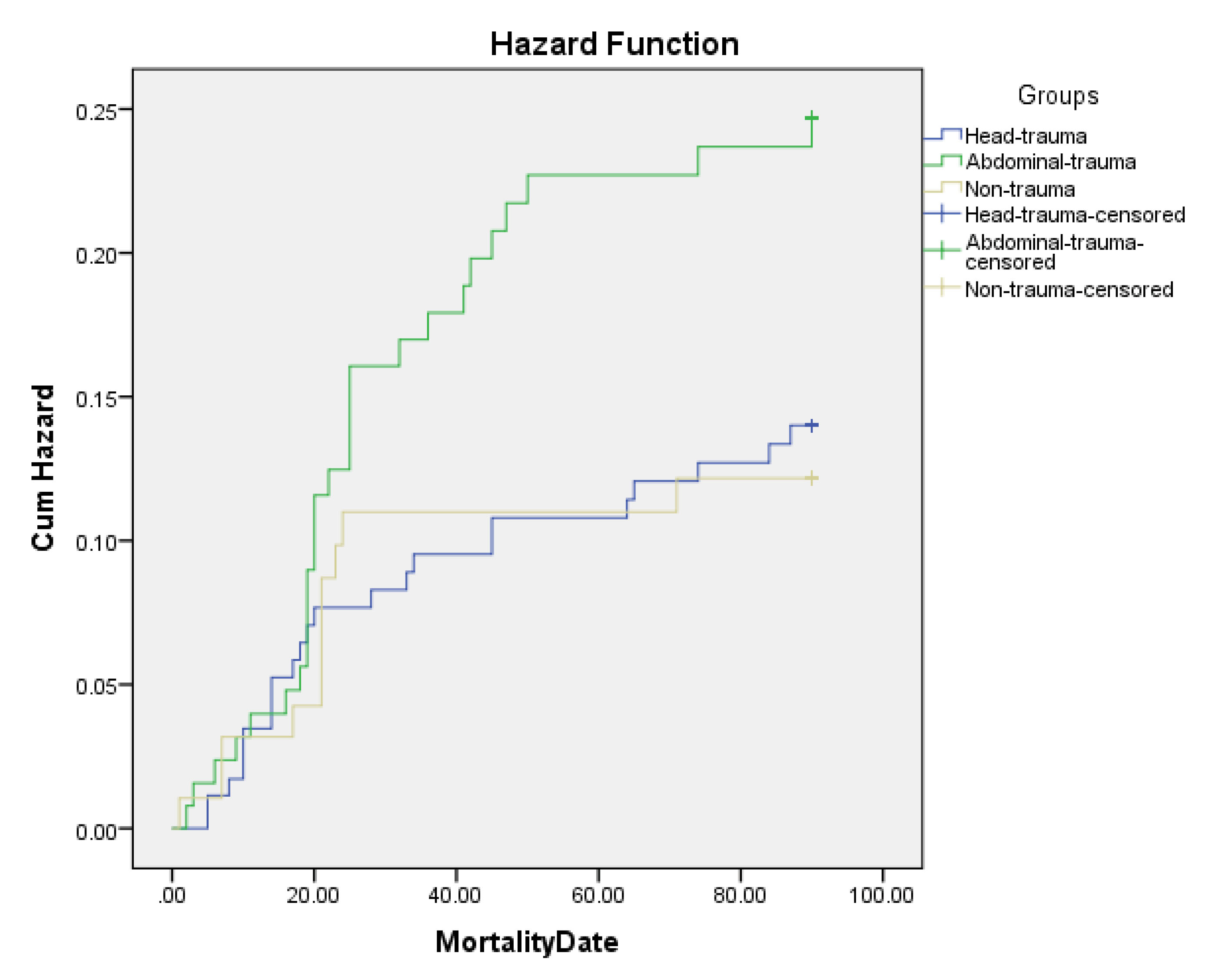
Figure 2.
Kaplan Meier Log-Rank Test for 90-Day Mortality Rates in the Three Study Groups.
.
Kaplan Meier Log-Rank Test for 90-Day Mortality Rates in the Three Study Groups.
Discussion
This is the first study to compare 90-day mortality in abdominal trauma with patients receiving intensive care in a general surgery ICU and head trauma patients. In the present study, significantly more males than females presented with abdominal trauma (82.8% vs 17.2%), such that the male-to-female ratio was 4.8:1. Our finding is consistent with studies conducted by Gad et al20 and Lone et al21 who reported a male to female ratio of 4.4:1 among abdominal trauma patients. The ratio of males to females is greater in the abdominal trauma group compared with the head trauma and surgical ICU patients where the ratio is more evenly matched. The mean age of included patients appears to be different when the abdominal trauma (24-45 years) and head trauma (18–56 years) groups are contrasted with the older surgical ICU population (28-66 years). Young males aged 24 to 30 years have been reported to be the most frequent victims.22 There is no question, because it is well-known that young men are more adventurous than others in any group of people. Males tend to experience abdominal injuries more frequently, but sex differences have not been demonstrated in the head trauma and surgical ICU patients groups. Therefore, the results of this analysis reflecting age and sex differences are expected, yet conclusions must be framed with the understanding that different physiologic processes are represented in each group.
Survival outcomes varied among our participants with higher mortality associated with abdominal trauma (21.9%) compared with the head trauma (13.1%) and surgical ICU (11.5%) groups. More than 50% of all deaths in the abdominal and head trauma groups occurred within 20 days after admission. Mean time to death was 27.85 ± 20.1, 30.27 ± 18.22 and 31.43 ± 26.24 days for abdominal trauma, surgical ICU, and head trauma groups, respectively. According to the average length of ICU stay for each group of patients, most deaths in the abdominal injuries group occurred in the first days after discharge from the ICU. This may suggest to focus more on the initial days after ICU discharge in terms of quality improvement. So, this patient population often require a multidisciplinary team to care for them both in the ICU and afterwards in the general ward.
The high mortality rate in patients with abdominal trauma can be due to a variety of reasons, including the extremely complex pathophysiology of abdominal injuries. These pathophysiologic events are common to both blunt and penetrating injury in response to hemorrhage, tissue injury, pain, thermal challenge, dysoxia or hypoxia, and acidosis.23-25 Patients with abdominal trauma are sometimes underestimated by their treating physicians due to seemingly less trauma and receive less intensive care and are discharged from the ICU prematurely, which increases the risk of death in these patients. Blunt abdominal trauma is more likely to be missed because clinical signs are less obvious.26 Diagnosis of abdominal trauma can often be challenging because it sometimes takes time for intra-abdominal injuries to become apparent.27 Several studies have shown that delayed arrival of the patient to the ED as well as pre-hospital care of trauma patients is very important and might contribute to the morbidity and mortality of abdominal trauma patients.28-31 On the other hand, unplanned discharges from the ICU at night-time and on weekends were independent risk factors for readmission to the ICU and increased mortality.32-34 Moreover, involvement of multiple organs in intra-abdominal injuries and the presence of associated extra-abdominal injuries in addition to abdominal injuries result in severe injuries and subsequently influence the patients’ outcomes.35-37 This evidence indicates the need for a coordinated trauma care system and properly trained personnel to take care of abdominal injuries in trauma patients. A team approach is essential for successful management of the injured patient. This team includes consulting physicians from various disciplines as well as physiatrists, nursing, physical and occupational therapy, respiratory therapy, nutrition, social work, and case management. Patients with abdominal injuries who need to be admitted to the ICU need follow-up and rehabilitation treatment after discharge, which seems necessary to shorten the recovery time and reduce the mortality rate in these patients.
There are several limitations to our study. Our study is a single-center study, and our results may be therefore not widely generalizable. Potential unmeasured confounders not included in our analysis may also be present. Furthermore, we did not distinguish between patients with blunt abdominal injuries and those with penetrating abdominal injuries. However, this study for the first time evaluated 90-day mortality in patients with abdominal trauma and compared it with the other two groups.
In conclusion, difficulty in accurate diagnosis due to the complex physiological variability of abdominal trauma, less obvious clinical symptoms in blunt abdominal injuries, multi-organ dysfunction in abdominal injuries, failure to provide timely acute care, as well as different treatment methods all account for the high 90-day mortality rate in patients with abdominal trauma compared to patients with head trauma and surgical ICU patients. Therefore, these patients need a multidisciplinary team to care for them both in the ICU and afterwards in the general ward. In addition, it seems necessary to follow these patients after discharge from the hospital as well as rehabilitation programs to shorten the recovery time and reduce the mortality rate in these patients.
Acknowledgements
Thanks to guidance and advice from the “Clinical Research Development Unit Be’sat Hospital” in Hamadan, Iran.
Authors’ Contribution
SJM and KGM conceived and designed the original protocol, supervised the study and interpreted the data. FRB and AFJ coordinated the study, enrolled the patients and performed the follow-up visits, and collected the data. SA entered and analyzed all the data and wrote the final draft of manuscript. FRB and SA wrote the first draft of the manuscript.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interest.
Ethical Statement
The research protocol was reviewed and approved by the Ethics Committee of Hamadan Medical University of Hamadan, Iran (IR.UMSHA. REC. 1400.340). Informed consent was obtained from all patients or, in cases where the patient is was unable to make a decision, from their legal guardian.
References
- Aldemir M, Taçyildiz I, Girgin S. Predicting factors for mortality in the penetrating abdominal trauma. Acta Chir Belg 2004; 104(4):429-34. [ Google Scholar]
- Arumugam S, Al-Hassani A, El-Menyar A, Abdelrahman H, Parchani A, Peralta R. Frequency, causes and pattern of abdominal trauma: a 4-year descriptive analysis. J Emerg Trauma Shock 2015; 8(4):193-8. doi: 10.4103/0974-2700.166590 [Crossref] [ Google Scholar]
- Karamercan A, Yilmaz TU, Karamercan MA, Aytaç B. Blunt abdominal trauma: evaluation of diagnostic options and surgical outcomes. Ulus Travma Acil Cerrahi Derg 2008; 14(3):205-10. [ Google Scholar]
- Smith J, Caldwell E, D’Amours S, Jalaludin B, Sugrue M. Abdominal trauma: a disease in evolution. ANZ J Surg 2005; 75(9):790-4. doi: 10.1111/j.1445-2197.2005.03524.x [Crossref] [ Google Scholar]
- Mehta N, Babu S, Venugopal K. An experience with blunt abdominal trauma: evaluation, management and outcome. Clin Pract 2014; 4(2):599. doi: 10.4081/cp.2014.599 [Crossref] [ Google Scholar]
- Pande R, Saratzis A, Winter Beatty J, Doran C, Kirby R, Harmston C. Contemporary characteristics of blunt abdominal trauma in a regional series from the UK. Ann R Coll Surg Engl 2017; 99(1):82-7. doi: 10.1308/rcsann.2016.0223 [Crossref] [ Google Scholar]
- Lotfollahzadeh S, Burns B. Penetrating abdominal trauma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2021.
- Siddharth BR, Keerthi MSS, Naidu SB, Venkanna M. Penetrating injuries to the abdomen: a single institutional experience with review of literature. Indian J Surg 2017; 79(3):196-200. doi: 10.1007/s12262-016-1459-0 [Crossref] [ Google Scholar]
- Naeem BK, Perveen S, Naeem N, Ahmed T, Khan I, Khan I. Visceral injuries in patients with blunt and penetrating abdominal trauma presenting to a tertiary care facility in Karachi, Pakistan. Cureus 2018; 10(11):e3604. doi: 10.7759/cureus.3604 [Crossref] [ Google Scholar]
- Hamsen U, Drotleff N, Lefering R, Gerstmeyer J, Schildhauer TA, Waydhas C. Mortality in severely injured patients: nearly one of five non-survivors have been already discharged alive from ICU. BMC Anesthesiol 2020; 20(1):243. doi: 10.1186/s12871-020-01159-8 [Crossref] [ Google Scholar]
- Agbroko S, Osinowo A, Jeje E, Atoyebi O. Determinants of outcome of abdominal trauma in an urban tertiary center. Niger J Surg 2019; 25(2):167-71. doi: 10.4103/njs.NJS_2_19 [Crossref] [ Google Scholar]
- Soni KD, Kaushik G, Gupta A, Singh V, Kumar S, Sagar S. From emergency department to intensive care unit, does the delay matter to trauma patients?. J Emerg Trauma Shock 2018; 11(3):189-92. doi: 10.4103/jets.jets_132_17 [Crossref] [ Google Scholar]
- Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systematic review and meta-analysis. Crit Care 2015; 19(1):254. doi: 10.1186/s13054-015-0973-y [Crossref] [ Google Scholar]
- Jung B, Daurat A, De Jong A, Chanques G, Mahul M, Monnin M. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med 2016; 42(4):494-504. doi: 10.1007/s00134-016-4254-2 [Crossref] [ Google Scholar]
- Barmparas G, Ley EJ, Martin MJ, Ko A, Harada M, Weigmann D. Failure to rescue the elderly: a superior quality metric for trauma centers. Eur J Trauma Emerg Surg 2018; 44(3):377-84. doi: 10.1007/s00068-017-0782-x [Crossref] [ Google Scholar]
- Stewart RM, Myers JG, Dent DL, Ermis P, Gray GA, Villarreal R. Seven hundred fifty-three consecutive deaths in a level I trauma center: the argument for injury prevention. J Trauma 2003; 54(1):66-70. doi: 10.1097/00005373-200301000-00009 [Crossref] [ Google Scholar]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008; 61(4):344-9. doi: 10.1016/j.jclinepi.2007.11.008 [Crossref] [ Google Scholar]
- Jiang H, Yao Z, Guo G, Wang Y, Li F. APACHE IV score is useful for assessment and stratification of elderly patients over 65 years with acute cholecystitis. Surg Laparosc Endosc Percutan Tech 2019; 29(6):524-8. doi: 10.1097/sle.0000000000000725 [Crossref] [ Google Scholar]
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13(10):818-29. [ Google Scholar]
- Gad MA, Saber A, Farrag S, Shams ME, Ellabban GM. Incidence, patterns, and factors predicting mortality of abdominal injuries in trauma patients. N Am J Med Sci 2012; 4(3):129-34. doi: 10.4103/1947-2714.93889 [Crossref] [ Google Scholar]
- Lone GN, Peer GQ, Wani K, Bhat AM, Wani NA, Bhat MA. An experience with abdominal trauma in adults in Kashmir. JK Pract 2001; 8(4):225-30. [ Google Scholar]
- Baradaran H, Salimi J, Nassaji-Zavareh M, Khaji A, Rabbani A. Epidemiological study of patients with penetrating abdominal trauma in Tehran-Iran. Acta Med Iran 2007; 45(4):305-8. [ Google Scholar]
- Feliciano DV. Abdominal trauma revisited. Am Surg 2017; 83(11):1193-202. [ Google Scholar]
- Geelhoed GW. Blunt and penetrating abdominal trauma. Am Fam Physician 1978; 17(3):96-104. [ Google Scholar]
- Eckert KL. Penetrating and blunt abdominal trauma. Crit Care Nurs Q 2005; 28(1):41-59. doi: 10.1097/00002727-200501000-00005 [Crossref] [ Google Scholar]
- Jansen JO, Yule SR, Loudon MA. Investigation of blunt abdominal trauma. BMJ 2008; 336(7650):938-42. doi: 10.1136/bmj.39534.686192.80 [Crossref] [ Google Scholar]
- Jones EL, Stovall RT, Jones TS, Bensard DD, Burlew CC, Johnson JL. Intra-abdominal injury following blunt trauma becomes clinically apparent within 9 hours. J Trauma Acute Care Surg 2014; 76(4):1020-3. doi: 10.1097/ta.0000000000000131 [Crossref] [ Google Scholar]
- Ntundu SH, Herman AM, Kishe A, Babu H, Jahanpour OF, Msuya D. Patterns and outcomes of patients with abdominal trauma on operative management from northern Tanzania: a prospective single centre observational study. BMC Surg 2019; 19(1):69. doi: 10.1186/s12893-019-0530-8 [Crossref] [ Google Scholar]
- Khashayar P, Ahmadi Amoli H, Tavakoli H, Panahi F. Efficacy of pre-hospital care in trauma patients in Iran. Emerg Med J 2010; 27(6):430-2. doi: 10.1136/emj.2008.071738 [Crossref] [ Google Scholar]
- Williamson K, Ramesh R, Grabinsky A. Advances in prehospital trauma care. Int J Crit Illn Inj Sci 2011; 1(1):44-50. doi: 10.4103/2229-5151.79281 [Crossref] [ Google Scholar]
- Beuran M, Paun S, Gaspar B, Vartic N, Hostiuc S, Chiotoroiu A. Prehospital trauma care: a clinical review. Chirurgia (Bucur) 2012; 107(5):564-70. [ Google Scholar]
- Azevedo LC, de Souza IA, Zygun DA, Stelfox HT, Bagshaw SM. Association between nighttime discharge from the intensive care unit and hospital mortality: a multi-center retrospective cohort study. BMC Health Serv Res 2015; 15:378. doi: 10.1186/s12913-015-1044-4 [Crossref] [ Google Scholar]
- Yang S, Wang Z, Liu Z, Wang J, Ma L. Association between time of discharge from ICU and hospital mortality: a systematic review and meta-analysis. Crit Care 2016; 20(1):390. doi: 10.1186/s13054-016-1569-x [Crossref] [ Google Scholar]
- Laupland KB, Shahpori R, Kirkpatrick AW, Stelfox HT. Hospital mortality among adults admitted to and discharged from intensive care on weekends and evenings. J Crit Care 2008; 23(3):317-24. doi: 10.1016/j.jcrc.2007.09.001 [Crossref] [ Google Scholar]
- El-Menyar A, Abdelrahman H, Al-Hassani A, Peralta R, AbdelAziz H, Latifi R. Single versus multiple solid organ injuries following blunt abdominal trauma. World J Surg 2017; 41(11):2689-96. doi: 10.1007/s00268-017-4087-3 [Crossref] [ Google Scholar]
- Karachentsev S. Blunt trauma to abdominal solid organs: an experience of non-operative management at a rural hospital in Zambia. Pan Afr Med J 2021; 38:89. doi: 10.11604/pamj.2021.38.89.20061 [Crossref] [ Google Scholar]
- Faist E, Baue AE, Dittmer H, Heberer G. Multiple organ failure in polytrauma patients. J Trauma 1983; 23(9):775-87. doi: 10.1097/00005373-198309000-00002 [Crossref] [ Google Scholar]