Arch Iran Med. 25(4):274-276.
doi: 10.34172/aim.2022.44
Case Report
A Patient with Acute Abdominal Pain Caused by an Unnoticed Swallowed Toothpick Misdiagnosed as Acute Appendicitis
Yong Yao 1  , Gaowu Yan 2, Lei Feng 1, *
, Gaowu Yan 2, Lei Feng 1, *
Author information:
1The Division of Gastroenterology and Hepatology, Suining Central Hospital, Suining City, Sichuan Province, China
2The Department of Radiology, Suining Central Hospital, Suining City, Sichuan Province, China
*
Corresponding Author: Lei Feng, MD; The Division of Gastroenterology and Hepatology, Suining Central Hospital, Suining City, Sichuan Province, China. Tel:+86-18008258982; Fax:+86-08252292270; Email:
fenglei822@163.com
Abstract
The differential diagnosis of acute abdominal pain is a challenging task for medical doctors working in the department of gastroenterology. It is clear that acute abdominal pain may be associated with a number of pathologic conditions. We report an unusual case of an unnoticed swallowed wooden toothpick stuck in the ileocecal area of a young man with right lower abdominal pain who was misdiagnosed as acute appendicitis. However, an abdominal computed tomography scan showed an elongated foreign body stuck in the ileocecal area. The elongated foreign body was identified as a wooden toothpick, which was then grasped with a foreign body forceps and successfully removed through colonoscopy. The patient’s abdominal pain was significantly relieved within 2 days following treatment. On the basis of the case report, we suggest the importance of abdominal computed tomography scans for the differential diagnosis of acute abdominal pain and highlight the need for extra vigilance in excluding the diagnosis of foreign bodies in the gastrointestinal tract of patients with acute abdominal pain.
Keywords: Acute abdominal pain, Acute appendicitis, Computed tomography, Differential diagnosis, Foreign body, Toothpick
Copyright and License Information
© 2022 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Yao Y, Yan G, Feng L. A patient with acute abdominal pain caused by an unnoticed swallowed toothpick misdiagnosed as acute appendicitis. Arch Iran Med. 2022;25(4):274-276. doi: 10.34172/aim.2022.44
Introduction
Acute abdominal pain is a common symptom among patients who present to the department of gastroenterology, which can be caused by various diseases, including acute appendicitis, bowel obstruction, nonspecific abdominal pain, acute diverticulitis and gastro-intestinal diseases.1 The different causes for acute abdominal pain can entail different prognoses, ranging from self-limiting to life-threatening processes among patients with acute abdominal pain.2 Acute appendicitis, a life-threatening disease, is manifested by acute right lower abdominal pain, fever, nausea, vomiting and diarrhea and often accompanied by the development of severe complications.3 Most patients with acute appendicitis require timely diagnosis and surgical treatment for better outcomes. However, the diagnosis of acute appendicitis is based on history and typical clinical symptoms and some diseases presenting as acute right lower abdominal pain may be easily mistaken for acute appendicitis.4 Here, we report a case of acute right lower abdominal pain due to an unnoticed swallowed toothpick, which was misdiagnosed as acute appendicitis and successfully treated by endoscopic removal of the toothpick.
Case Report
A 27-year-old young man was admitted to our hospital as a patient presenting with a 3-day history of right lower abdominal pain and diarrhea. He had a 10-pack-year history of cigarette smoking and a history of habitual heavy alcohol intake of more than 70 g/d. The rest of the patient’s history, family history, developmental history, social history, and review of systems was unremarkable. Physical examination showed that he had a normal body temperature and localized right lower abdominal tenderness with mild rebound tenderness, but no guarding. Blood counts revealed a mild leukocytosis 11.5 × 109/L, with predominant neutrophils (76.2%) with normal platelet count and hemoglobin. Plasma high-sensitivity C-reactive protein was increased at 2.99 mg/dL. Computed tomography (CT) of the abdomen without contrast media revealed swelling of the ileocecal mucosa. Other laboratory tests and conventional radiological examinations were normal. Therefore, a primary diagnosis of acute appendicitis was made based on his history and clinical examination findings. However, his infections were unapparent or mild, and thus, he underwent a contrast-enhanced CT scan of the abdomen. Interestingly, the CT scan of the abdomen revealed the presence of an elongated foreign body in the ileocecal area (Figures 1A and 1B). Accordingly, the patient was examined by colonoscopy and the results of colonoscopy showed a wooden toothpick stuck in the ileocecal area (Figure 1C). The wooden toothpick was then grasped with a foreign body forceps and successfully removed through colonoscopy (Figure 1D). The young man was unaware of ever having swallowed a wooden toothpick, but remembered that he had pitched up food with a toothpick in a state of drunkenness 3 days ago. The patient’s abdominal pain was significantly relieved within 2 days following treatment.
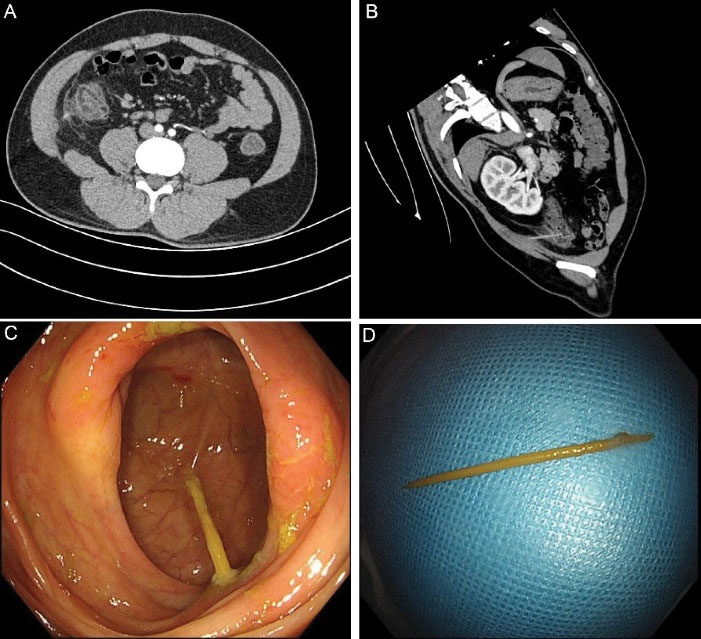
Figure 1.
A Toothpick Stuck in the Ileocecal Region of a Patient with Right Lower Quadrant Abdominal Pain. (A) CT scan of the abdomen reveals a foreign body. (B) CT scan sagittal reconstruction image shows a high-density needle-shaped structure in the ileocecal area. (C) Endoscopic view of the toothpick stuck in the ileocecal area. (D) Photograph of the removed wooden toothpick.
.
A Toothpick Stuck in the Ileocecal Region of a Patient with Right Lower Quadrant Abdominal Pain. (A) CT scan of the abdomen reveals a foreign body. (B) CT scan sagittal reconstruction image shows a high-density needle-shaped structure in the ileocecal area. (C) Endoscopic view of the toothpick stuck in the ileocecal area. (D) Photograph of the removed wooden toothpick.
Discussion
Here, we report a rare case of foreign body stuck in the ileocecal area, which was misdiagnosed as acute appendicitis. Various laboratory tests and radiological examinations are available to assist the diagnosis of acute appendicitis, but none of them are specific for the documentation of acute appendicitis.5,6 Therefore, the differential diagnosis of acute appendicitis is challenging, especially in young women for whom there is a larger range of differential diagnoses than for men.7 Gottschalk et al reported a case of an incarcerated uterus in a patient presenting at 24 weeks’ gestation with severe bilateral flank and lower abdominal pain who was initially misdiagnosed as acute appendicitis.8 For this reason, acute appendicitis should be diagnosed by ruling out other causes of right lower abdominal pain. CT is an important tool in the diagnosis and differential diagnosis of acute appendicitis.9-11 Sinnott andHowlett reported a case of a 38-year-old man with acute appendicitis who presented with atypical clinical symptoms and underwent a CT scan, which showed a dilated, thick walled appendix, confirming the diagnosis of acute appendicitis.12 Previous studies for patients with acute appendicitis have shown that CT has a high level of diagnostic accuracy that is unaffected by the percentage of female participants, adopted scanning protocol or patient presentation. CT has proven to be more accurate in the diagnosis of acute appendicitis than ultrasonography and has specificity and sensitivity rates between 83–100% and 76–100%.13 Abdominal CT scan in patients with suspected acute appendicitis can significantly reduce the rate of negative appendectomy, which is as high as 15%.14 Accordingly, abdominal CT should be performed as a routine preoperative procedure in all patients with suspected acute appendicitis.
In our patient, abdominal CT was performed to reveal that right lower abdominal pain in this patient was likely the result of an elongated foreign body stuck in the ileocecal area and colonoscopy confirmed that the foreign body was a wooden toothpick. So far, a number of case reports have presented the cases of foreign bodies in the gastrointestinal tract of patients with various clinical manifestations. Venkatesan et al reported a case of pyogenic hepatic abscess secondary to gastric perforation caused by an ingested fish bone.15 Unexpectedly, a mobile phone was found in the stomach of a 39-year-old man.16 To the best of our knowledge, ours is the first report to present a case of an unnoticed swallowed wooden toothpick stuck in the ileocecal area of a young man with right lower abdominal pain who was misdiagnosed as acute appendicitis. Because the small intestine of an adult is about 6.4 meters long, a swallowed toothpick is often difficult to reach the ileocecal area through the small intestine. A previously published study reported a patient who suffered from a toothpick stuck in small intestine,17 but in our case, the toothpick reached the ileocecal area.
In conclusion,this case emphasizes the importance of an abdominal CT scan in the clinical treatment of abdominal pain. In addition, the diagnosis of foreign bodies in the gastrointestinal tract should be considered in the differential diagnosis of abdominal pain.
Acknowledgements
This work was supported by the Medical science program of Sichuan province of China (Number Q18048) and the science program of Health Commission of Sichuan Province of China (Number 20PJ286).
Authors’ Contribution
We took turns in caring for the patient. YY acquired the data and figures and produced a first draft of this report. GY analysed the figures. LF reviewed and polished the manuscript.
Conflict of Interest Disclosures
The authors declare no conflicts of interest.
Disclaimer
The case report has not been presented or published in any conference or any other journal.
Ethical Statement
The patient signed a written informed consent for using any data for research and educational purposes. Also, the ethical committee letter was duly signed for the case report from the concerned department.
References
- Gans SL, Pols MA, Stoker J, Boermeester MA. Guideline for the diagnostic pathway in patients with acute abdominal pain. Dig Surg 2015; 32(1):23-31. doi: 10.1159/000371583 [Crossref] [ Google Scholar]
- Laméris W, van Randen A, van Es HW, van Heesewijk JP, van Ramshorst B, Bouma WH. Imaging strategies for detection of urgent conditions in patients with acute abdominal pain: diagnostic accuracy study. BMJ 2009; 338:b2431. doi: 10.1136/bmj.b2431 [Crossref] [ Google Scholar]
- Kleif J, Kirkegaard A, Vilandt J, Gögenur I. Randomized clinical trial of preoperative dexamethasone on postoperative nausea and vomiting after laparoscopy for suspected appendicitis. Br J Surg 2017; 104(4):384-92. doi: 10.1002/bjs.10418 [Crossref] [ Google Scholar]
- Baird DLH, Simillis C, Kontovounisios C, Rasheed S, Tekkis PP. Acute appendicitis. BMJ 2017; 357:j1703. doi: 10.1136/bmj.j1703 [Crossref] [ Google Scholar]
- Bhangu A. Evaluation of appendicitis risk prediction models in adults with suspected appendicitis. Br J Surg 2020; 107(1):73-86. doi: 10.1002/bjs.11440 [Crossref] [ Google Scholar]
- Theilen LH, Mellnick VM, Shanks AL, Tuuli MG, Odibo AO, Macones GA. Acute appendicitis in pregnancy: predictive clinical factors and pregnancy outcomes. Am J Perinatol 2017; 34(6):523-8. doi: 10.1055/s-0036-1593764 [Crossref] [ Google Scholar]
- Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet 2015; 386(10000):1278-87. doi: 10.1016/s0140-6736(15)00275-5 [Crossref] [ Google Scholar]
- Gottschalk EM, Siedentopf JP, Schoenborn I, Gartenschlaeger S, Dudenhausen JW, Henrich W. Prenatal sonographic and MRI findings in a pregnancy complicated by uterine sacculation: case report and review of the literature. Ultrasound Obstet Gynecol 2008; 32(4):582-6. doi: 10.1002/uog.6121 [Crossref] [ Google Scholar]
- Cartwright SL, Knudson MP. Diagnostic imaging of acute abdominal pain in adults. Am Fam Physician 2015; 91(7):452-9. [ Google Scholar]
- Schifeling CH, Williams DA. Appropriate use of imaging for acute abdominal pain. JAMA Intern Med 2017; 177(12):1853-4. doi: 10.1001/jamainternmed.2017.6135 [Crossref] [ Google Scholar]
- Bachur RG, Rangel SJ. The threat of diagnostic uncertainty in the medical management of uncomplicated appendicitis. JAMA Pediatr 2017; 171(6):505-6. doi: 10.1001/jamapediatrics.2017.0053 [Crossref] [ Google Scholar]
- Sinnott JD, Howlett DC. A man with severe abdominal pain. BMJ 2016; 353:i2379. doi: 10.1136/bmj.i2379 [Crossref] [ Google Scholar]
- Gorter RR, Eker HH, Gorter-Stam MA, Abis GS, Acharya A, Ankersmit M. Diagnosis and management of acute appendicitis. EAES consensus development conference 2015. Surg Endosc 2016; 30(11):4668-90. doi: 10.1007/s00464-016-5245-7 [Crossref] [ Google Scholar]
- National Surgical Research Collaborative. Multicentre observational study of performance variation in provision and outcome of emergency appendicectomy. Br J Surg 2013; 100(9):1240-52. doi: 10.1002/bjs.9201 [Crossref] [ Google Scholar]
- Venkatesan S, Falhammar H. Pyogenic hepatic abscess secondary to gastric perforation caused by an ingested fish bone. Med J Aust 2019;211(10):451-451.e1. 10.5694/mja2.50395
- Milivojevic V, Rankovic I, Milic L, Jeremic V, Jovanovic I. Mobile phone in the stomach: call the emergency endoscopist!. Gastrointest Endosc 2017; 86(1):233-4. doi: 10.1016/j.gie.2016.10.030 [Crossref] [ Google Scholar]
- Gray DM, To K, Wang JS. Toothpick perforation of the small bowel. Clin Gastroenterol Hepatol 2011; 9(11):A26. doi: 10.1016/j.cgh.2011.05.013 [Crossref] [ Google Scholar]