Arch Iran Med. 24(9):704-705.
doi: 10.34172/aim.2021.102
Photoclinic
Bronchial Dieulafoy lesion: A mimic of tracheal tumor
Hang Ruan  , Jian Zhu , Ying-Nan Wang *
, Jian Zhu , Ying-Nan Wang *
Author information:
1Department of Pulmonary and Critical Care Medicine, The People’s Hospital of China Three Gorges University, Yichang, China
*Corresponding Author: Ying-Nan Wang, MD; Department of Pulmonary and Critical Care Medicine, The People’s Hospital of China Three Gorges University, 4 Huti Street, 443000 Yichang, Hubei, China. Tel: +98-13-886665333; Email:
ycwyn@163.com
Copyright and License Information
© 2021 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Ruan H, Zhu J, Wang Y. Photoclinic. Arch Iran Med. 2021;24(9):704-705. doi: 10.34172/aim.2021.102
A 52-year-old patient was admitted to our hospital with a seven-day history of recurrent hemoptysis. The clinical symptoms occurred occasionally, producing up to 15 mL of sputum stained with fresh blood after coughing. She had no history of an underlying disease. A physical examination of the lung revealed rough breathing sounds in the lungs. The laboratory findings revealed no obvious abnormal values, including for liver and renal function, C-reactive protein and complete blood count. Bronchoscopy confirmed the presence of an ileal mass with rich vascularity (Figure 1). Chest computed tomography (CT) showed a mass protruding into the airway lumen (Figure 2). After enhancement, homogeneous enhancement was observed in the areas (Figure 3).
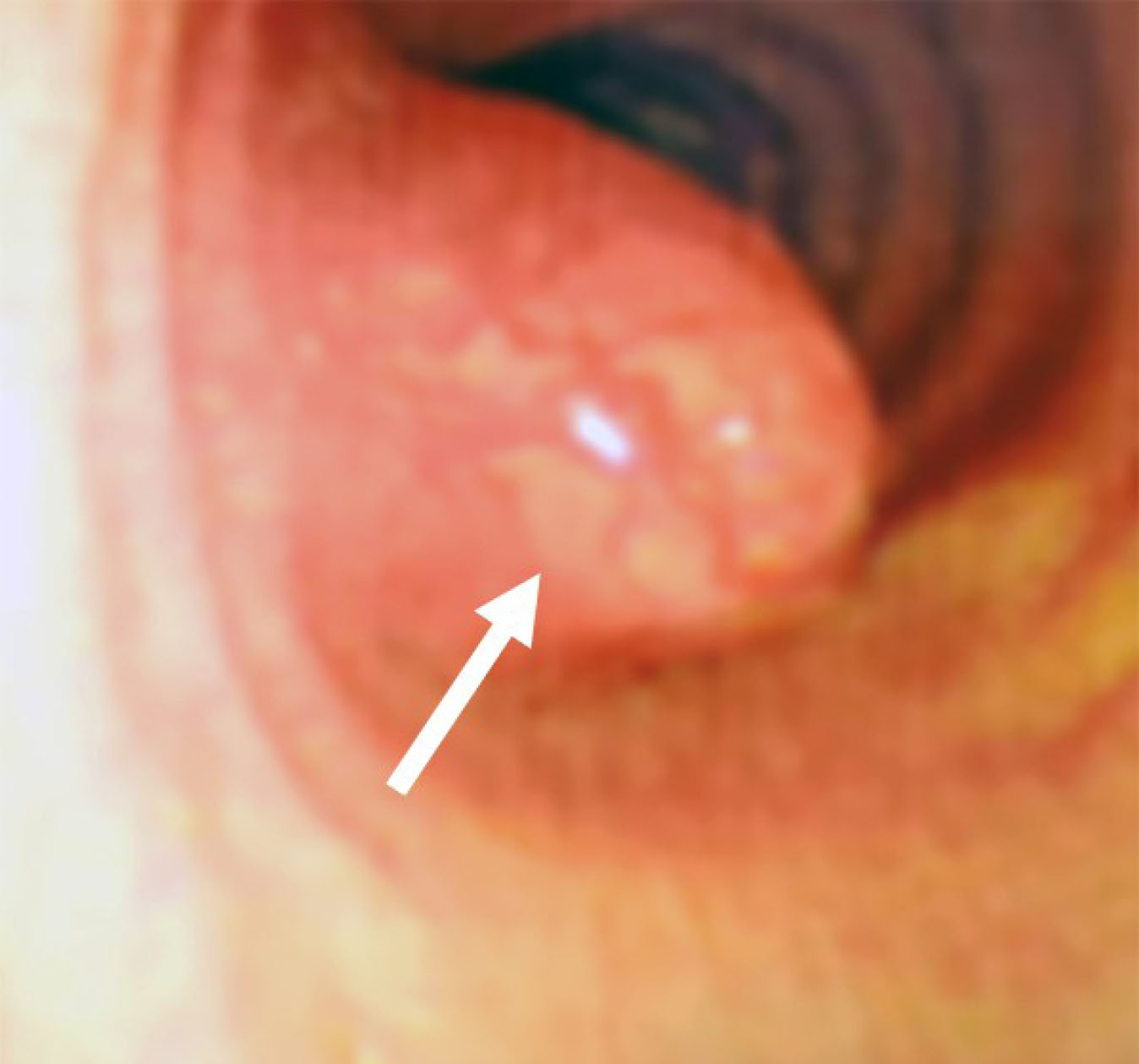
Figure 1.
Bronchoscopy examination revealed a smooth mass at the 9 o’clock position in the trachea (white arrow).
.
Bronchoscopy examination revealed a smooth mass at the 9 o’clock position in the trachea (white arrow).

Figure 2.
Chest computed tomography showing low-density mass protruding into the airway lumen (white arrow).
.
Chest computed tomography showing low-density mass protruding into the airway lumen (white arrow).

Figure 3.
After enhancement, homogeneous enhancement was observed in the areas (white arrow).
.
After enhancement, homogeneous enhancement was observed in the areas (white arrow).
Photoclinic Diagnosis
Dieulafoy’s disease had been defined as vascular malformation in the past and was thought to originate only from the gastrointestinal tract.1 However, a bronchial Dieulafoy lesion was first described in 1955 by the British pathologist Sweerts in the form of vascular malformation in the bronchi.2 Pathologically, the lesions, localized in the submucosal tissue of the trachea, typically appear as a dilated and tortuous artery that abuts the margin of the membranous tracheal wall. The vascular anomalies may originate from a bronchial artery or pulmonary artery.3
The latest studies describe the endoscopic findings in favor of Bronchial Dieulafoy lesion as (a) a smooth mass protruding into the respiratory tract with clear boundaries, (b) enlarged and ectatic blood vessels observed and extending into the subserosa, and (c) mostly on the right side.
According to the existing literature, the medical management of Bronchial Dieulafoy lesions includes surgical repair, endoscopic treatment, and vascular embolization.4 Angiography and embolization could be helpful for the control of bronchial artery malformation. Endovascular intervention is generally considered ineffective for these vascular anomalies, supplied from pulmonary artery circulation entirely. Such patients are usually referred for endoscopic treatment or surgery. Our patient underwent bronchial artery embolization with resolution of symptoms.
Authors’ Contribution
HR and JZ participated in collection and interpretation of data, literature search, and writing the manuscript. YNW was involved in reviewing the manuscript.
Conflict of Interest Disclosures
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical Statement
In writing the manuscript, the authors followed the policy of the Committee on Publication Ethics (COPE).
References
- Inayat F, Amjad W, Hussain Q, Hurairah A. Dieulafoy’s lesion of the duodenum: a comparative review of 37 cases. BMJ Case Rep 2018; 2018. doi: 10.1136/bcr-2017-223246 [Crossref]
- Sweerts M, Nicholson AG, Goldstraw P, Corrin B. Dieulafoy’s disease of the bronchus. Thorax 1995; 50(6):697-8. doi: 10.1136/thx.50.6.697 [Crossref] [ Google Scholar]
- Tang P, Wu T, Li C, Lv C, Huang J, Deng Z. Dieulafoy disease of the bronchus involving bilateral arteries: a case report and literature review. Medicine (Baltimore) 2019; 98(44):e17798. doi: 10.1097/md.0000000000017798 [Crossref] [ Google Scholar]
- Baghai Wadji M, Farahzadi A. Dieulafoy’s disease of the bronchial tree: a case report. Sao Paulo Med J 2017; 135(4):396-400. doi: 10.1590/1516-3180.2016.0258191116 [Crossref] [ Google Scholar]