Arch Iran Med. 25(5):300-307.
doi: 10.34172/aim.2022.49
Original Article
Validation of Persian Version of Mindful Attention Awareness Scale (MAAS) in Iranian Women with Breast Cancer
Roghieh Nooripour 1  , Nikzad Ghanbari 2, Peyman Hassani-Abharian 3, * , Laurel E. Radwin 4, Simin Hosseinian 1, Saba Hasanvandi 5
, Nikzad Ghanbari 2, Peyman Hassani-Abharian 3, * , Laurel E. Radwin 4, Simin Hosseinian 1, Saba Hasanvandi 5
Author information:
1Department of Counseling, Faculty of Education and Psychology, Alzahra University, Tehran, Iran
2Faculty of Education and Psychology, Shahid Beheshti University (SBU), Tehran, Iran
3Institute for Cognitive Science Studies (IRICSS), Department of Cognitive Rehabilitation, Brain and Cognition Clinic, Tehran, Iran
4Center for Health Care Organizational and Implementation Research (CHOIR), VA Boston Healthcare System, Boston, MA, USA
5Department of Psychology, Faculty of Humanistic Sciences, Khorramabad Branch, Islamic Azad University, Khorram Abad, Iran
*
Corresponding Author: Peyman Hassani-Abharian, MD, PhD; Assistant professor in Institute for Cognitive Science Studies, Brain and Cognition Clinic, Tehran, Iran. Email:
abharian1972@yahoo.com &
abharian@iricss.org
Abstract
Background:
Breast cancer is now the most significant health issue in women, threatening diverse aspects of human health, including mental health and cognitive function. This research aimed to validate the Persian version of Mindful Attention Awareness Scale (MAAS) in Iranian women with breast cancer.
Methods:
We gathered data on 229 women with breast cancer in Tehran through convenience sampling. They completed a demographic questionnaire, the Persian version of MAAS, the General Self-Efficacy Scale, and DASS-21. SPSS-22 analyzed the Pearson correlation between the Persian version of MAAS, general self-efficacy, and DASS-21. Also, LISREL 8.8 was used to analyze the internal structure of the MAAS.
Results:
Findings from the confirmatory factor analysis (CFA) showed that the model with one factor fits well with the data (sbχ2=4.29 (P=0.36); SRMR=0.058; CFI=1.0; NFI=0.91; IFI=0.95; RFI=0.97; GFI=0.90; RMSEA=0.069). Significant negative correlations were found between MAAS and DASS-21 scores for anxiety (r=-0.51), depression (r=-0.48) and stress (r=-0.49), indicating an acceptable divergent validity. There was also a positive relationship between MAAS and general self-efficacy (r=0.37; P<0.01).
Conclusion:
The Persian version of MAAS seems to be a valid scale for evaluating the extent of mindfulness of Iranian women with breast cancer.
Keywords: Breast cancer, Iranian women, Mindful Attention Awareness Scale (MAAS), Mindfulness
Copyright and License Information
© 2022 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article as: Nooripour R, Ghanbari N, Hassani-Abharian P, Radwin LE, Hosseinian S, Hasanvandi S. Validation of persian version of mindful attention awareness scale (maas) in iranian women with breast cancer. Arch Iran Med. 2022;25(5):300-307. doi: 10.34172/aim.2022.49
Introduction
Breast cancer is now the most significant health issue in women, threatening diverse aspects of human health, including mental health and cognitive function. It has been estimated that 2.4 million women died of this disease between 1999 and 2015.1 More than 1.5 million women (25% of all women with cancer) worldwide are diagnosed with breast cancer.2 This disease has spread equally throughout the world.3 In 2019, after lung cancer, breast cancer was the second most common type of cancer in women.4
Cancer is a life-threatening illness that causes over 6.7 million deaths per year.5 Some risk factors, including gender, age, estrogen, history of family, genetic defects, and unhealthy lifestyles, may increase the disease incidence.6 Several factors contribute to this type of cancer, such as urbanization and unhealthy nutrition habit. So, healthy nutrition and a healthy lifestyle have been identified as preventive factors.7
Emotional and psychological issues can arise in women with breast cancer, such as insomnia, anorexia, suicidal thinking, fear of cancer recurrence, and fear of death. Up to one-third of breast cancer patients may experience mental illness more than one year after the initial surgery.8 In the last 12 years, related post-traumatic stress symptoms have been identified one year after surgery. Unwanted side effects of adjuvant cancer therapy may also play a moderating role, despite complications for many years following treatment in a large proportion of women. Psychosocial factors may serve as mental illness mediators.9
Considering the health, psychological, social, and functional problems of women with breast cancer,10,11 it is necessary to design and use precise instruments to assess patients’ cognitive, behavioral, and physical symptoms. Some psychometric instruments have been developed to assess, diagnose, and help reduce cognitive and behavioral problems, such as stress, in cancer patients,12 for example, mindfulness has been found to reduce stress symptoms and affect beneficial immunological and endocrine changes in cancer patients.13,14
Recently, despite increasing clinical research, there have been very few mindfulness assessments and thus no method of evaluating whether some interventions such as Mindfulness Based Stress Reduction (MBSR) effectively promote progress in the mindfulness level. The initial self-reporting measures of mindfulness that have been developed are listed in chronological order: (1) Freiburg Mindfulness Inventory (FMI),15 which had one factor and was developed by meditation practitioners and explicitly designed for meditation experience, which would make it challenging to be applied to individuals who do not practice meditation. FMI is a 30-item tool for evaluating moment-by-moment observation and openness to a negative experience and is designed for experienced meditators. (2) Mindful Attention Awareness Scale (MAAS),16 a comprehensive overview is included in this article, which also describes why this has been chosen. (3) Kentucky Inventory of Mindfulness Skills (KIMS),17 which includes three different subscales measuring different mindfulness skills, namely, observe, describe, and act with awareness. KIMS is a practical and constructive measure for professionals involved in teaching mindfulness skills to their patients. 4) Cognitive and Affective Mindfulness Scale (CAMS),18 although not a mindfulness scale, evaluates attention, awareness, acceptance, and present focus. (5) Toronto Mindfulness Scale (TMS),19 a concise one-factor scale, was initially developed to be used in combination with meditation. TMS is a 10-item, single-factor tool measuring conscious mindfulness during an instant meditation exercise. (6) Five Facets Mindfulness Questionnaire (FFMQ).20 Some specialists have developed FFMQ based on five additional subjectivity assessment measures, including FMI, MAAS, KIMS, CAMS, and MQ. After carrying out the analysis, it was determined that the mindfulness construct is based on five different constructs. It was concluded that mindfulness is not a one-factor structure but involves factors like “describing/labeling with words.” (7) Southampton Mindfulness Questionnaire (SMQ),21 a range intended to measure the awareness of unsettling ideas and pictures. This particular scale was initially designed for psychosis patients. (8) Philadelphia Mindfulness Scale,22 a two-dimensional measure that evaluates two elements of mindfulness; present-moment awareness and acceptance that are not necessarily related. Although each tool uses its terms to explain and understand mindfulness, and while there is a wide overlap between theories, based on the varying results of these different studies, more research is required to determine whether the instrument assesses mindful attention awareness accurately.
In this regard, one of the most widely used clinical instruments is the MAAS.23 It is ideal for assessing focus and perception of the momentary experience of real-life a larger community.
MAAS is a 15-item self-report measure prepared by Brown and Ryan16 to evaluate mindfulness. They showed its efficacy in assessing motivation and health that improved MAAS preoperative perception assessment in a limited sample of cancer patients in an MBSR sample was correlated with decreased mood disturbances and stress.
MAAS is a one-factorial perception of a structure, focusing on variable attention/awareness in the present moment as an integral feature of the mind. The MAAS scale is a quick and easy test that assesses a person’s capacity to be receptive and attentive to a single factor in experiencing the present moment of everyday life.16 Using MAAS does not mean that the person has already meditated, and the basic formula has strong psychometric properties. These characteristics make MAAS the most common tool in research studies to assess mindfulness, such as in depression,24 stress,25 bulimia,26 chronic pain,27 or cancer.28
Although clinical populations, including women with breast cancer, require careful evaluation, this scale has few psychometric assessments among cancer patients, especially patients with breast cancer. This raises the question of whether MAAS-assessed alertness is valid in clinical populations compared to observations in populations where the instrument is validated. This is essential given the recognized need for validated mindfulness measures and related research. Moreover, to our knowledge, MAAS has not yet been validated for breast cancer in Iranian women, and this is the first attempt to validate it. Therefore, the current study aimed to evaluate the MAAS psychometric assessment for Iranian women with breast cancer.
Materials and Methods
Participants
The current study is a descriptive-analytical study in Tehran from November 2018 to April 2019. Sampling was done through a convenience method. As some studies had suggested a total of 200–300 for factor analysis to be acceptable,29 229 women with breast cancer were finally selected.
We focused on the research question to determine which criteria are crucial for participants to meet to help the study collect the most significant results. Inclusion criteria were age 20 to 70 years, breast cancer in stages 1, 2, or 3, the ability to read and write, no history of specific diseases, and willingness to participate in the research activities. Exclusion criteria were incomplete questionnaire response and reluctance to participate in the study, other types of malignancy, and disease duration less than two months.
Instruments
The researchers employed a demographic characteristics checklist to gather data on marital status, educational status, age group, tumor stage, tumor treatment, and time to diagnosis (days).
Mindful Attention Awareness Scale
This measure consists of a 15-item that uses a 6-point Likert scale from 1 (nearly always) to 6 (nearly never). Total ratings vary from 15 to 90, with higher scores indicating higher rates of mindfulness. Respondents are asked to read every item and report their daily life experiences. In Iran, Cronbach’s alpha was at 0.90 for the non-clinical population.30
General Self-Efficacy Scale
The scale was developed in 1979 by Schwarzer and Jerusalem and revised in 1981 to have ten items, all of which measure general self-efficacy. The score is based on a four-point Likert scale ranging from 1 to 4, with scores of 10 to 20 showing low self-efficacy, between 21 and 30 showing mild self-efficacy, and scores above 30 showing high self-efficacy. Cronbach’s alpha has been reported at 0.82.31 In Iran, Cronbach’s alpha was obtained to be 0.81.32
Depression, Anxiety, and Stress Scale-21 Items (DASS-21)
In 1995, Lovibond and Lovibond developed a 21-item scale to assess stress, anxiety, and depression. Each question’s score ranged from zero (it does not happen to me at all or never) to 3 (much or often applicable to me). A validity of 0.77 was reported for this scale by Brown et al.33 Each subscale contained seven items whose final score could be obtained by summing the items’ scores to vary from 0 to 21 per sub-scale. In Iran, the reliability of DASS-21 was measured at 0.82 using the Cronbach’s alpha method.34
Procedure
This research was divided into two sections: instrument’s translation and cultural adaptation strategies, so MAAS was translated into Farsi (Persian) in the first phase using the back-translation technique, and the second was the assessment of its validity. A sample of 53 patients was used to assess temporal consistency. Finally, no Persian word was unclear for the patients, so no adjustments were made to the translated scale in the final Persian edition of MAAS. Moreover, reliability was estimated by test-retest and Guttman split-half coefficient.
Statistical Analysis
Normality was tested by the Kolmogorov-Smirnov test, which indicated that the variable follows a normal distribution (P > 0.05). Demographic characteristics and the Pearson correlation between the Persian version of MAAS, self-efficacy, and DASS-21 were analyzed. Confirmatory factor analysis (CFA) was performed to determine the convergent and discriminant validity. Convergent validity refers to how closely the current scale applies to other factors and other measurements of the same construct. Not only does the construct correlate with relevant variables, but it should not correlate with different, unrelated variables. The determination in the last lines has been referred to as discriminative validity.35,36 The single-factor structure was used to analyze the internal structure of the MAAS by LISREL 8.8.
Results
Descriptive Statistic
The participants’ age ranged from 20 to 70 years (Mean = 36.7, SD = 9.24). MAAS’s mean (SD) was calculated at 58.46 (12.72). Cronbach’s alpha for MAASwas0.86 (CI = 0.82–0.89). There was a significant relationship (P < 0.001) between MAAS and educational status. Table 1 indicates the correlation between MAAS and socio-demographic and clinical features.
Table 1.
Correlation between MAAS with the Socio-demographic and Clinical Characteristic
|
|
N
|
%
|
M
|
SD
|
F
|
P
|
| Marital status |
|
|
|
|
1.43 |
0.22 |
| Married |
108 |
47.57 |
59.73 |
13.46 |
| Single/widowed, divorced |
119 |
52.42 |
57.31 |
11.94 |
| Educational status |
|
|
|
|
7.4 |
0.001
|
| Under diploma |
53 |
23.34 |
56.07 |
14.33 |
| Diploma |
77 |
33.92 |
55.50 |
11.68 |
| Above diploma |
97 |
42.73 |
62.11 |
11.74 |
| Age group |
|
|
|
|
1.09 |
0.33 |
| ≤ 45 |
79 |
34.80 |
57.09 |
12.11 |
| 46–70 |
92 |
40.52 |
59.82 |
11.81 |
| ≥ 71 |
56 |
24.66 |
58.21 |
12.42 |
| Tumor stage |
|
|
|
|
0.43 |
0.66 |
| I–II |
129 |
56.82 |
58.15 |
12.02 |
| III |
98 |
43.17 |
58.86 |
12.37 |
| Tumor treatment |
|
|
|
|
0.97 |
0.33 |
| Chemotherapy |
126 |
55.51 |
57.74 |
11.96. |
| Chemo-radiotherapy |
101 |
44.49 |
59.35 |
12..89 |
| Time to diagnosis(days) |
|
|
|
|
0.42 |
0.67 |
| 0–60 |
132 |
58.14 |
58.75 |
12.05 |
| > 60 |
95 |
41.85 |
58.05 |
12.97 |
Bold values indicate the significance at the 5% level.
Confirmatory Factor Analysis
The results of CFA for MAAS are shown in Figure 1 and Table 2. The CFA findings for a single factor structure are illustrated in Table 3. These findings were reliable in terms of all items.
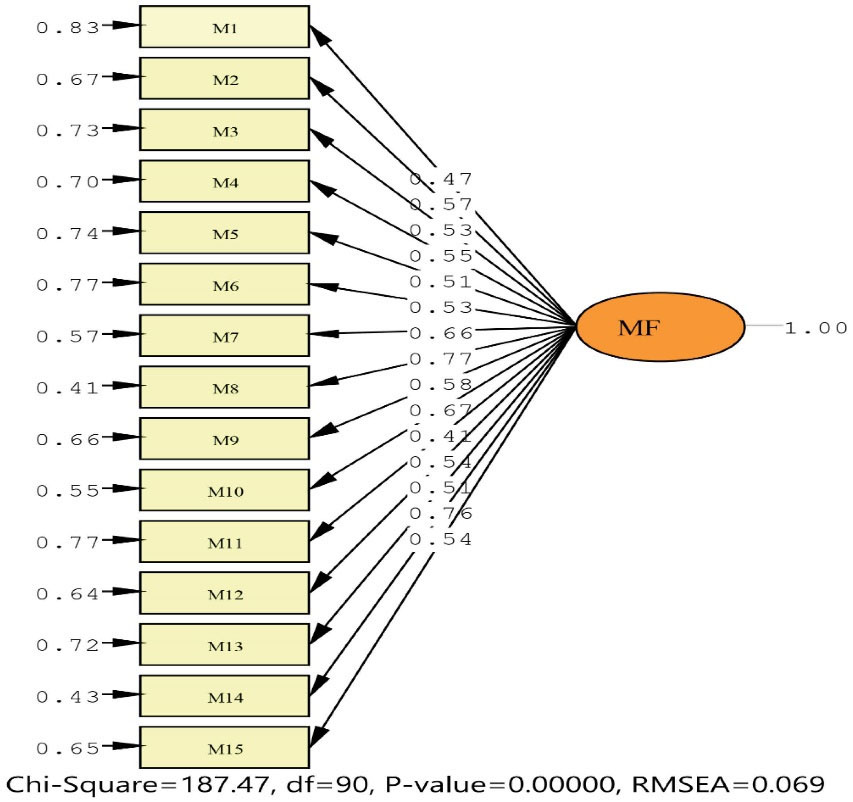
Figure 1.
Confirmatory Factor Analysis of Mindful Attention Awareness Scale.
.
Confirmatory Factor Analysis of Mindful Attention Awareness Scale.
Table 2.
Descriptive Statistics for all MAAS Items
|
Items
|
Items Statistics
|
Item-Total Statistics
|
|
M
|
SD
|
FL
|
V
|
IT
|
CD
|
SK
|
K
|
| Item 1 |
3.77 |
1.30 |
0.47 |
151.29 |
0.276 |
0.852 |
0.339 |
-0.829 |
| Item 2 |
4.50 |
1.42 |
0.57 |
141.37 |
0.543 |
0.838 |
-0.584 |
-0.658 |
| Item 3 |
3.80 |
1.44 |
0.53 |
143.15 |
0.480 |
0.842 |
-0.039 |
-0.978 |
| Item 4 |
3.69 |
1.53 |
0.55 |
140.70 |
0.518 |
0.839 |
-0.016 |
-1.123 |
| Item 5 |
3.92 |
1.56 |
0.51 |
145.37 |
0.371 |
0.848 |
-0.168 |
-1.136 |
| Item 6 |
4.36 |
1.54 |
0.53 |
143.78 |
0.423 |
0.845 |
-0.455 |
-1.086 |
| Item 7 |
4.06 |
1.54 |
0.66 |
137.40 |
0.612 |
0.834 |
-0.273 |
-1.097 |
| Item 8 |
4.11 |
1.49 |
0.77 |
135.89 |
0.680 |
0.830 |
-0.237 |
-1.104 |
| Item 9 |
3.86 |
1.55 |
0.58 |
140.18 |
0.523 |
0.839 |
-0.234 |
-1.019 |
| Item 10 |
3.97 |
1.53 |
0.67 |
137.19 |
0.618 |
0.834 |
-0.212 |
-1.120 |
| Item 11 |
2.95 |
1.41 |
0.41 |
153.53 |
0.179 |
0.857 |
0.453 |
-0.600 |
| Item 12 |
4.27 |
1.51 |
0.54 |
141.49 |
0.500 |
0.841 |
-0.425 |
-0.869 |
| Item 13 |
2.58 |
1.43 |
0.51 |
146.66 |
0.377 |
0.847 |
0.728 |
-0.086 |
| Item 14 |
3.91 |
1.51 |
0.76 |
135.85 |
0.671 |
0.831 |
-0.119 |
-1.136 |
| Item 15 |
4.64 |
1.50 |
0.54 |
143.50 |
0.445 |
0.844 |
-0.867 |
-0.385 |
M, mean; SD, standard deviation; FL, factor loadings; V, scale variance if item deleted; I.T., corrected item-total correlations; C.D., Cronbach’s alpha if item deleted; SK, Skewness; K, Kurtosis.
The model’s fit indices were evaluated: Root mean square error of approximation (RMSEA; criterion < 0.08) and its 90% confidence, standardized root mean square residual (SRMR; criterion < 0.09), root mean square residual (RMR; criterion < 0.050), comparative fit index (CFI; criterion > 0.90), normed fit index (NFI; criterion > 0.90), incremental fit index (IFI; criterion > 0.90), relative fit index (RFI; criterion > 0.90), adjusted goodness of fit index (AGFI; criterion > 0.80), goodness of fit index (GFI; criterion > 0.90). CFA showed that single factor structure provided a good fit to the data: sbχ2 = 187.47 (P= 0.001); SRMR = 0.058; CFI = 0.95; NFI = 0.91; IFI = 0.95; RFI = 0.90; AGFI = 0.87; GFI = 0.90; RMSEA = 0.069. All items of loads show a significant factor, as shown in Table 3.
Table 3.
Model Fit Index
|
sb
X
2
|
SRMR
|
CFI
|
NFI
|
IFI
|
RFI
|
AGFI
|
GFI
|
RMSEA
|
| 187.47 |
0.058 |
0.95 |
0.91 |
0.95 |
0.90 |
0.87 |
0.90 |
0.069 |
SRMR, standardized root mean squared residual; CFI, comparative fit index; NFI, normed fit index; IFI, incremental fit index; RFI, relative fit index; GFI, goodness-of-fit index; RMSEA, root mean square error of approximation.
Divergent and Convergent Validity
There was a significant negative relationship between MAAS and DASS-21 (depression: r = -0.48, < 0.001; stress: r = -.49, P < 0.001; anxiety: r = -0.51, P < 0.001; and total score: r = 0.52, P < 0.001). There was a significant and positive relationship between MAAS and self-efficacy (r = 0.37; P < 0.001). These findings illustrate acceptable divergent and convergent validity for MAAS (Table 4).
Table 4.
Pearson’s Correlation Between MAAS and DASS-21
|
|
Mean (SD)
|
1
|
2
|
3
|
4
|
5
|
6
|
| 1. MAAS |
58.46 (12.72) |
1 |
|
|
|
|
|
| 2. DASS-21, Depression |
17.93 (4.12) |
-0.48** |
0.1 |
|
|
|
|
| 3. DASS-21, Stress |
18.92 (3.72) |
-0.49** |
0.43** |
1 |
|
|
|
| 4. DASS-21, Anxiety |
15.81 (3.85) |
-0.51** |
0.35** |
0.18* |
0.1 |
|
|
| 5. DASS-21, Total |
52.66 (8.59) |
-0.53** |
0.77** |
0.69** |
0.66** |
1 |
|
| 6. Self-efficacy |
27.32 (6.21) |
0.37** |
-0.41** |
-0.29** |
-0.18* |
-0.33** |
1 |
MAAS, Version of Mindful Attention Awareness Scale; DASS, Depression, Anxiety, and Stress Scale.
*
P ≤ 0.05; **P ≤ 0.01.
Temporal Validity
A sample of 53 patients were used to assess temporal consistency, and the findings revealed that after two weeks, the coefficient of test and re-test was 0.81 (CI = 0.70–0.75).
Discussion
This study demonstrated that the Persian version of MAAS is acceptable in Iranian women with breast cancer to measure mindfulness. There was a significant correlation between the level of education and MAAS throughout our research. Moreover, CFA indicated that higher education level plays a role in increasing women’s awareness of breast cancer among demographic variables. Also, the divergent validity between MAAS with DASS-21 was significantly negative, while the correlation between mindfulness and self-efficacy was positive.
MAAS has been validated in different clinical populations, such as cancer populations in other countries.37 Previous findings have also found that higher scores on this single factor mindfulness measure are correlated with a low mood disorder and student stress.16 Growing research has shown that mindfulness could be used widely in many diseases, particularly cancer. The nature of the disease is such that acute stress impairs the patient’s individual and sometimes social functioning and may exacerbate the course of the disease.38
There is a consensus that women have a vast spectrum of physical and mental symptoms over life.39 Epidemiologic research has shown several efforts to classify likely symptomatological effects through aging, endocrine modifications, demographics, psychosocial causes, environmental circumstances, cultural disparities, and differences across countries.40
Psychological stress, chronic exhaustion, discomfort, nausea, hair loss, body image disorders, and cognitive decline have been reported by cancer patients.41
Mental and physical conditions and many cancer therapies such as surgery, radiotherapy, chemotherapy, and hormone therapy may affect patients’ family, work, social relationships, and sexual function.42 One-third of cancer patients with mental conditions such as anxiety and depression are reported to be dealing with higher percentages of women and youth.43 There is also an increasing interest in mindfulness research, especially in oncology situations, to be aware of life stressors such as cancer diagnosis.44
From the cognitive and behavioral point of view, reducing the psychological burden of cancer through cognitive rehabilitation techniques such as mindfulness, in the long run, raises the resilience of the affected women. All variables investigated in this study played an important role in predicting the efficacy of cognitive rehabilitation techniques such as mindfulness. The final model also showed that the higher the education level of the affected women, the more they benefit from the mindfulness technique. Mindfulness can promote different cognitive functions such as retention, thinking, problem-solving, and emotional balance, and these components seem to be better developed in educated women.
Some studies have shown that mindfulness training could increase awareness and attention in students.45 Among clinical populations, such as breast cancer patients, only the educated could increase the performance of this instrument. In other words, present-moment attention and acting with awareness have been more prominent in educated people.
It is suggested that this study be conducted on different types of cancers and different stages separately to determine the scale’s sensitivity to it. It is also recommended that this study be repeated by changing the population to other chronic diseases. Also, longitudinal research with this scale in women with cancer is recommended to assess their mindful attention awareness.
While there were strengths in the present study, limitations were also notable. One of the limitations of the present study is that it is limited to women with cancer, limiting generalizability to other statistical populations. Due to the lack of random sampling, generalization of the findings to other populations must be made with caution. So, this scale must be validated in different environments and on different samples in future research. Second, mindfulness is subjective, and it has limitations in its critical measurement. The nature of self-reports fails to eliminate the likelihood of answers influenced by social attractiveness considerations.
The present study also confirmed that the items used are appropriate, and the questionnaire retains its structure without any possible changes or omissions. Another point is that the cultural and racial differences and different Iranian sample experiences did not cause mindfulness to be evaluated differently from the English language sample. In explaining this issue, we can point to the spiritual context of mindfulness and, consequently, the non-cultural and universal nature of spirituality, free from racial and cultural differences. There is a need for spirituality in all places and times, and spirituality can be defined as a quality beyond gender, nationality, ethnicity, and any other difference.
This research was done on Iranian women with breast cancer. Future studies can validate the Persian version of MAAS among the general and clinical populations. In practice, this study offers a robust forum for the therapeutic use of MAAS. In potential simulations, though, other latent variables could be possible. Therefore, it is recommended to use other latent variables for future studies. Finally, the validity of Persian MAAS has only started to be evaluated by current research, and future studies could measure the size of useful experimental, neurological, and behavioral findings.
As a result, the Persian version of MAAS is a helpful tool to measure individual differences in the ability to pay attention and be mindful of momentary experiences among Iranian women with breast cancer; therefore, this scale can be used to evaluate the results of treatments and attention and awareness at the present moment.
Acknowledgements
The authors appreciate the participants for their kindness and patience.
Authors’ Contribution
All of the authors provided an equal level of contribution to the study.
Conflict of Interest Disclosures
None.
Ethical Statement
All methods have been carried out under relevant guidelines and regulations. All research procedures involving humans were consistent with the National Research Committee’s ethical standards, the Helsinki Declaration of 1964, subsequent revisions, or equivalent ethical norms. Before inclusion, all participants signed informed consent forms.
References
- La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F. Thyroid cancer mortality and incidence: a global overview. Int J Cancer 2015; 136(9):2187-95. doi: 10.1002/ijc.29251 [Crossref] [ Google Scholar]
- McGuire S. World Cancer Report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, WHO Press, 2015. Adv Nutr 2016; 7(2):418-9. doi: 10.3945/an.116.012211 [Crossref] [ Google Scholar]
- Shankar A, Saini D, Roy S, Mosavi Jarrahi A, Chakraborty A, Bharti SJ. Cancer care delivery challenges amidst coronavirus disease - 19 (COVID-19) outbreak: specific precautions for cancer patients and cancer care providers to prevent spread. Asian Pac J Cancer Prev 2020; 21(3):569-73. doi: 10.31557/apjcp.2020.21.3.569 [Crossref] [ Google Scholar]
- Nooripour R, Hosseinian S, Ghanbari N, Haghighat S, Matacotta JJ, Gasparri ML. Validation of the Persian version of the satisfaction with life scale (SWLS) in Iranian women with breast Cancer. Curr Psychol. 2021:1-8. 10.1007/s12144-021-01662-2
- DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA Cancer J Clin 2016; 66(1):31-42. doi: 10.3322/caac.21320 [Crossref] [ Google Scholar]
- Nielsen SM, White MG, Hong S, Aschebrook-Kilfoy B, Kaplan EL, Angelos P. The breast-thyroid cancer link: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 2016; 25(2):231-8. doi: 10.1158/1055-9965.epi-15-0833 [Crossref] [ Google Scholar]
- Johnson CB, Davis MK, Law A, Sulpher J. Shared risk factors for cardiovascular disease and cancer: implications for preventive health and clinical care in oncology patients. Can J Cardiol 2016; 32(7):900-7. doi: 10.1016/j.cjca.2016.04.008 [Crossref] [ Google Scholar]
- Nosarti C, Roberts JV, Crayford T, McKenzie K, David AS. Early psychological adjustment in breast cancer patients: a prospective study. J Psychosom Res 2002; 53(6):1123-30. doi: 10.1016/s0022-3999(02)00350-1 [Crossref] [ Google Scholar]
- Morgans AK, Fan KH, Koyama T, Albertsen PC, Goodman M, Hamilton AS. Influence of age on incident diabetes and cardiovascular disease in prostate cancer survivors receiving androgen deprivation therapy. J Urol 2015; 193(4):1226-31. doi: 10.1016/j.juro.2014.11.006 [Crossref] [ Google Scholar]
- Li Y, Qiao Y, Luan X, Li S, Wang K. Family resilience and psychological well-being among Chinese breast cancer survivors and their caregivers. Eur J Cancer Care (Engl) 2019; 28(2):e12984. doi: 10.1111/ecc.12984 [Crossref] [ Google Scholar]
- Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology 2001; 10(1):19-28. doi: 10.1002/1099-1611(200101/02)10:1<19::aidpon501>3.0.co;2-6 [Crossref] [ Google Scholar]
- Andic F, Miller AH, Brown G, Chu L, Lin J, Liu T. Instruments for determining clinically relevant fatigue in breast cancer patients during radiotherapy. Breast Cancer 2020; 27(2):197-205. doi: 10.1007/s12282-019-01008-8 [Crossref] [ Google Scholar]
- Nooripour R, Ghanbari N, Hoseinian S, Vakili Y, Dobkins K. Psychometric validation of the Farsi version of the Mindful Attention Awareness Scale (MAAS) in a sample of Iranian students in the USA. Int J Ment Health Addict. 2021. 10.1007/s11469-021-00617-9
- Speca M, Carlson LE, Goodey E, Angen M. A randomized, wait-list controlled clinical trial: the effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosom Med 2000; 62(5):613-22. doi: 10.1097/00006842-200009000-00004 [Crossref] [ Google Scholar]
- Walach H, Buchheld N, Buttenmüller V, Kleinknecht N, Schmidt S. Measuring mindfulness—the Freiburg Mindfulness Inventory (FMI). Pers Individ Dif 2006; 40(8):1543-55. doi: 10.1016/j.paid.2005.11.025 [Crossref] [ Google Scholar]
- Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol 2003; 84(4):822-48. doi: 10.1037/0022-3514.84.4.822 [Crossref] [ Google Scholar]
- Baer RA, Smith GT, Allen KB. Assessment of mindfulness by self-report: the Kentucky Inventory of Mindfulness Skills. Assessment 2004; 11(3):191-206. doi: 10.1177/1073191104268029 [Crossref] [ Google Scholar]
- Hayes AM, Feldman G. Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy. Clin Psychol (New York) 2004; 11(3):255-62. doi: 10.1093/clipsy.bph080 [Crossref] [ Google Scholar]
- Lau MA, Bishop SR, Segal ZV, Buis T, Anderson ND, Carlson L. The Toronto Mindfulness Scale: development and validation. J Clin Psychol 2006; 62(12):1445-67. doi: 10.1002/jclp.20326 [Crossref] [ Google Scholar]
- 20 Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006; 13(1):27-45. doi: 10.1177/1073191105283504 [Crossref] [ Google Scholar]
- Chadwick P, Hember M, Symes J, Peters E, Kuipers E, Dagnan D. Responding mindfully to unpleasant thoughts and images: reliability and validity of the Southampton Mindfulness Questionnaire (SMQ). Br J Clin Psychol 2008; 47(Pt 4):451-5. doi: 10.1348/014466508x314891 [Crossref] [ Google Scholar]
- Cardaciotto L, Herbert JD, Forman EM, Moitra E, Farrow V. The assessment of present-moment awareness and acceptance: the Philadelphia Mindfulness Scale. Assessment 2008; 15(2):204-23. doi: 10.1177/1073191107311467 [Crossref] [ Google Scholar]
- MacKillop J, Anderson EJ. Further psychometric validation of the Mindful Attention Awareness Scale (MAAS). J Psychopathol Behav Assess 2007; 29(4):289-93. doi: 10.1007/s10862-007-9045-1 [Crossref] [ Google Scholar]
- Christopher MS, Gilbert BD. Incremental validity of components of mindfulness in the prediction of satisfaction with life and depression. Curr Psychol 2010; 29(1):10-23. doi: 10.1007/s12144-009-9067-9 [Crossref] [ Google Scholar]
- Shapiro SL, Brown KW, Thoresen C, Plante TG. The moderation of mindfulness-based stress reduction effects by trait mindfulness: results from a randomized controlled trial. J Clin Psychol 2011; 67(3):267-77. doi: 10.1002/jclp.20761 [Crossref] [ Google Scholar]
- Lavender JM, Jardin BF, Anderson DA. Bulimic symptoms in undergraduate men and women: contributions of mindfulness and thought suppression. Eat Behav 2009; 10(4):228-31. doi: 10.1016/j.eatbeh.2009.07.002 [Crossref] [ Google Scholar]
- Cusens B, Duggan GB, Thorne K, Burch V. Evaluation of the breathworks mindfulness-based pain management programme: effects on well-being and multiple measures of mindfulness. Clin Psychol Psychother 2010; 17(1):63-78. doi: 10.1002/cpp.653 [Crossref] [ Google Scholar]
- Labelle LE, Campbell TS, Carlson LE. Mindfulness-based stress reduction in oncology: evaluating mindfulness and rumination as mediators of change in depressive symptoms. Mindfulness 2010; 1(1):28-40. doi: 10.1007/s12671-010-0005-6 [Crossref] [ Google Scholar]
- Byrne BM. Factor analytic models: viewing the structure of an assessment instrument from three perspectives. J Pers Assess 2005; 85(1):17-32. doi: 10.1207/s15327752jpa8501_02 [Crossref] [ Google Scholar]
- Ghorbani N, Watson PJ, Weathington BL. Mindfulness in Iran and the United States: cross-cultural structural complexity and parallel relationships with psychological adjustment. Curr Psychol 2009; 28(4):211. doi: 10.1007/s12144-009-9060-3 [Crossref] [ Google Scholar]
- Chang SH, Crogan NL, Wung SF. The self-care self-efficacy enhancement program for Chinese nursing home elders. Geriatr Nurs 2007; 28(1):31-6. doi: 10.1016/j.gerinurse.2006.11.006 [Crossref] [ Google Scholar]
- Moeini B, Shafii F, Hidarnia A, Babaii GR, Birashk B, Allahverdipour H. Perceived stress, self-efficacy and its relations to psychological well-being status in Iranian male high school students. Soc Behav Pers 2008; 36(2):257-66. doi: 10.2224/sbp.2008.36.2.257 [Crossref] [ Google Scholar]
- Brown TA, Chorpita BF, Korotitsch W, Barlow DH. Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behav Res Ther 1997; 35(1):79-89. doi: 10.1016/s0005-7967(96)00068-x [Crossref] [ Google Scholar]
- Asghari A, Saed F, Dibajnia P. Psychometric properties of the Depression Anxiety Stress Scales-21 (DASS-21) in a non-clinical Iranian sample. Int J Psychol 2008; 2(2):82-102. [ Google Scholar]
- Hubley AM, Zumbo BD. Psychometric characteristics of assessment procedures: an overview. In: Geisinger KF, Bracken BA, Carlson JF, Hansen JI, Kuncel NR, Reise SP, et al, eds. APA Handbook of Testing and Assessment in Psychology, Vol. 1: Test Theory and Testing and Assessment in Industrial and Organizational Psychology. American Psychological Association; 2013. p. 3-19. 10.1037/14047-001
- Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health 2018; 6:149. doi: 10.3389/fpubh.2018.00149 [Crossref] [ Google Scholar]
- Carlson LE, Brown KW. Validation of the Mindful Attention Awareness Scale in a cancer population. J Psychosom Res 2005; 58(1):29-33. doi: 10.1016/j.jpsychores.2004.04.366 [Crossref] [ Google Scholar]
- Cordova MJ, Riba MB, Spiegel D. Post-traumatic stress disorder and cancer. Lancet Psychiatry 2017; 4(4):330-8. doi: 10.1016/s2215-0366(17)30014-7 [Crossref] [ Google Scholar]
- Avis NE, Kaufert PA, Lock M, McKinlay SM, Vass K. The evolution of menopausal symptoms. Baillieres Clin Endocrinol Metab 1993; 7(1):17-32. doi: 10.1016/s0950-351x(05)80268-x [Crossref] [ Google Scholar]
- Dennerstein L, Dudley EC, Hopper JL, Guthrie JR, Burger HG. A prospective population-based study of menopausal symptoms. Obstet Gynecol 2000; 96(3):351-8. doi: 10.1016/s0029-7844(00)00930-3 [Crossref] [ Google Scholar]
- Dooley LN, Slavich GM, Moreno PI, Bower JE. Strength through adversity: moderate lifetime stress exposure is associated with psychological resilience in breast cancer survivors. Stress Health 2017; 33(5):549-57. doi: 10.1002/smi.2739 [Crossref] [ Google Scholar]
- Ord AS, Stranahan KR, Hurley RA, Taber KH. Stress-related growth: building a more resilient brain. J Neuropsychiatry Clin Neurosci 2020; 32(3):A4-212. doi: 10.1176/appi.neuropsych.20050111 [Crossref] [ Google Scholar]
- Hajian S, Mehrabi E, Simbar M, Houshyari M. Coping strategies and experiences in women with a primary breast cancer diagnosis. Asian Pac J Cancer Prev 2017; 18(1):215-24. doi: 10.22034/apjcp.2017.18.1.215 [Crossref] [ Google Scholar]
- Haller H, Winkler MM, Klose P, Dobos G, Kümmel S, Cramer H. Mindfulness-based interventions for women with breast cancer: an updated systematic review and meta-analysis. Acta Oncol 2017; 56(12):1665-76. doi: 10.1080/0284186x.2017.1342862 [Crossref] [ Google Scholar]
- de Bruin EI, Meppelink R, Bögels SM. Mindfulness in higher education: awareness and attention in university students increase during and after participation in a mindfulness curriculum course. Mindfulness 2015; 6(5):1137-42. doi: 10.1007/s12671-014-0364-5 [Crossref] [ Google Scholar]